Effective vaccines for COVID-19 raise the potential of disease eradication (elimination at the global level). Adapt Research contributed to a recent blog that considers the advantages and the challenges of eradication. Progressive expansion of “green zones” provide the best chance of eradicating COVID-19 and achieving the associated medium and long-term benefits. Full blog hosted externally, click here to continue reading.
The World Health Organization (WHO) needs a more proactive and transparent Emergency Committee to raise the alarm in health crises
Potentially catastrophic disease outbreaks must trigger a fire alarm, because humans resist action unless a piercing alarm is sounding
New international structures for rapid high-level propagation of the alarm are needed to ensure hasty responses
It will be necessary to have false alarms to ensure all true threats are detected
WHO pandemic advice should be tailored to contexts (eg island nations), rather than one-size-fits-all
WHO? The Emergency Committee
The international health regulations (IHR) provide for the Emergency Committee of the World Health Organization (WHO) to declare a Public Health Emergency of International Concern (PHEIC) in appropriate circumstances.
PHEIC is meant to be a signal to all countries that significant actions, aid and cooperation may all be needed. Critics have lambasted the late timing of PHEIC declaration for COVID-19 and also the opaque nature of the acronym.
SARS is specifically named in the IHR as a virus of significant concern. The world saw in 2003 how SARS coronaviruses can behave. Surely there was a strong argument for convening the Emergency Committee as early as 1 January 2020 and declaring a PHEIC immediately. We argue this point in our research letter published 23 February 2021.
Unfortunately, key information appears to have been suppressed in Wuhan during December 2019 leading to continued widespread travel in and out of the region throughout January.
With a more flexible decision-making process, able to countenance disparate and informal information sources (WeChat, Google, ProMed, Twitter), and with a mandate to investigate to verify concerning information, things might have been different for the Emergency Committee, and the world.
We need a fire alarm
Entities like the WHO Emergency Committee are fearful of unnecessarily alarming the world, so they remain silent for too long. Their function is analogous to a fire alarm, they are supposed to warn us loud and clear of imminent emergency. But fire alarmsdon’t actually tellus when there is a fire, as Eliezer Yudkowsky has explained. More times than not when a fire alarm sounds there is no fire, and this is how it must be. The threshold for alarm must be set below the threshold for risk so that the alarm sounds for all actual fires. Missing even one fire ends in ruin. The WHO Emergency Committee clearly missed a fire all through January 2020.
The mere sight of smoke (think snippets of information appearing on ProMed, or WeChat, or sidebar news stories) is not enough to compel people to act. This is especially true in a crowded world because of psychological barriers such as the bystander effect (surely someone else will act! I don’t want to look silly…).
Fire alarms give permission to act. If the alarm sounds, it’s OK to leave the building. It’s OK to get the extinguisher. It’s OK to close borders to arrivals from a disease epicentre. It’s OK to put masks on in public. You’re not going to look silly, because the alarm is sounding.
Well-functioning alarms activate at a low threshold and early enough that the fire can still be extinguished. The alarm must be piercing enough that normal activity cannot continue until the alarm is off. Alarms can be switched off right away if there is no evidence of a fire, but the fire brigade has to have time to check the building first.
A case in point was Auckland in February 2021. The city was put into a three-day lockdown in response to three community cases of COVID-19. Some critics said, with hindsight, that it was a ‘false alarm’ and complained that the government was too hasty. But the sight of people suddenly wearing masks, social distancing, and getting COVID tests because of the lockdown ‘alarm’ shows that fire alarms have a purpose. The brigade checked the building, and the alarm was quickly switched off.
PHEIC and prejudice
The issues surrounding the failures of the PHEIC alarm system are discussed in more depth in a podcast published by Nature. In sum there probably should be:
More powers to investigate/respond to non-official data on outbreaks
A ‘traffic light’ system so that PHEIC isn’t simply ‘yes’ or ‘no’, giving the Emergency Committee more powers to raise alert levels early on.
An international Pandemic Treaty
Reduction in Incentives to NOT report outbreaks (due to fear of economic harm if hotspots are then avoided – perhaps a compensation system could be workable?)
Incentives for countries to WANT to set up long-term systems and care about monitoring
Incentives for countries to agree to do these things
An industrial inferno: Global catastrophic biological risks
COVID-19 is a serious smouldering house fire, needing constant vigilance to put out hotspots. The next pandemic could be an industrial inferno.
There is a significant difference between a virus that causes fewer than 1% of those infected to die and one that causes 10%, 20%, 50% or more to die. Higher case fatality risk than COVID-19, or even higher than SARS (2003), poses the risk of a global biological catastrophe that overwhelms human systems and devastates society.
In our research letter, we argue that not only should PHEIC be declared much earlier, but that it should be declared ‘with-‘ or ‘without-‘ catastrophic risk. This might be the impetus for even stronger initial measures (such as Wuhan-style lockdowns, or border closure for island nations) right at the outset, with a realistic chance of eliminating the outbreak before it becomes a pandemic.
As successive instances of community transmission and the alert level system in several countries have shown, an initial overreaction can always be swiftly downgraded as information comes to light, but the reverse is not possible.
Pandemic advice: one size does not fit all
Initial and ongoing advice by the WHO following the PHEIC declaration was not context specific. For example, though possibly in line with evidence at the time for some contexts, advising against travel restrictions was completely inappropriate for small island nations. Perhaps even larger island nations such as the UK should have closed borders and pursued an elimination strategy for COVID-19. The UK faces obvious additional hurdles to the success of such a strategy, including dense connections to continental Europe, close proximity to other landmass making non-commercial sea and air access easy, as well as a huge logistical challenge and high probability of quarantine failures. That said, it may not be impossible and the debate was presented in The Guardian.
International cooperation is needed
Former New Zealand prime minister Helen Clark is leading an independent investigation into the global response to COVID-19. Speaking at the University of Otago, Wellington, on 1 Feb 2021, she indicated that a number of her recommendations, forthcoming in May, will centre around strengthening global institutions and connecting top-level decision makers. These connections will facilitate the functions that the world expects of these institutions.
A summary of her talk was published in The Conversation. Clark emphasised that nations must stop trying to go it alone. There is a strong case for multilateralism and the world needs to remove obstacles to a precautionary approach that were evident in China in December 2019, and within the WHO in January 2020.
At the Davos 2021 meeting, Ursula von der Leyen (President of the European Commission) delivered a speech noting that Europe is proposing a biodefense preparedness programme to sit within the new European Health Emergency Response Authority (HERA). The programme will scan for pathogens and prepare vaccines, with long-term predictable funding and public-private partnership. Earlier detection and faster scaling of response is needed. These are positive steps.
However, the solution, according to Helen Clark, must be global, and may need to include a high-level pandemic council consisting of the UN Secretary General, the WHO Director General, and the heads of the IMF and World Bank. This council can immediately agree on a course of action then use their influence to directly contact heads of state, finance ministers, and health ministers to coordinate a response. New Zealand could advocate for such a Council so that it is no longer a cork bobbing in the ocean of audacious whims of individualist global leaders, awaiting the sound of an alarm that will legitimise the necessary drastic action.
After the world failed to contain the 2003 SARS outbreak and it became a pandemic, the 2005 international health regulations (IHR) were born. The IHR included a mandate to report any cases of certain diseases (including SARS) to the World Health Organization (WHO) within 24 hours. Importantly the IHR requires all countries to be capable of preventing, detecting and responding to health emergencies.
Non-Compliance
Prevention and detection clearly failed at the outset for COVID-19. There is some evidence that a censured laboratory report identifying ‘SARS coronavirus’ emerged at Wuhan Central Hospital on 30 Dec 2019. Given the mandate to notify cases of SARS, and given the 2003 experience of a SARS pandemic, the WHO should have been able to declare a public health emergency of international concern (PHEIC) then and there. That did not happen. As it transpired a lack of Chinese transparency, politicisation, and reluctance to report the facts meant that the outbreak was not prevented, nor appropriately detected.
However, the IHR also mandates that countries ensure they are prepared to respond to global health threats. But once COVID-19 spread outside of China we saw how unprepared the world truly was.
This had been known for years. In 2012 only 42 of 194 States Parties to the IHR had self-reported compliance. This meant that 152 countries were not prepared to prevent, detect, or respond to significant health threats. Given the self-reported nature of the evidence, the reality may have been much worse. Two initiatives followed:
Invest and Measure
(1) the Global Health Security Agenda (GHSA) – a collaboration among many nations to enhance health security through investment and knowledge sharing, where notably the US invested nearly $1 billion in the health security of 31 developing nations.
(2) the Joint External Evaluations (JEE) with the WHO, whereby countries assessed their progress in conjunction with external teams, resulting in recommendations.
By 2018 only a minority of countries had yet undergone a JEE. Furthermore, it is apparent that many other factors contribute to health security beyond being prepared to prevent, detect and respond to outbreaks. For example, the quality of the health system and health workforce, the degree to which countries comply with international norms, and the risk environment. The world needed a universal and comprehensive measure of health security to identify gaps and target efforts.
The Global Health Security Index
The Global Health Security Index (GHSI) is such a tool and was used to measure health security capability of 195 countries across 140 items in 2019. The average global score was 40.2/100.
However, to be useful any measure of health security must be valid.
The GHSI has face validity, being the culmination of a programme of work that began with a systematic search for factors that underpin health security.
GSHI correlates strongly with measures of the JEE and so is useful for countries that have not yet undergone a JEE.
GHSI correlates moderately with aggregate mortality from communicable diseases suggesting that increasing GHSI might improve disease outcomes.
Countries that received US health security investments have higher GHSI (perhaps indicating the effectiveness of these investments).
GHSI scores are typically higher for countries with past domestic cases of SARS (indicating that countries might learn from prior outbreaks).
Overall, we found that the GHSI is a somewhat valid measure of health security, that is perhaps best used by countries to identify gaps in health security that might warrant further analysis. This is exactly what the authors of the original GHSI report concluded in the same recent issue of BMJ Global Health: The value proposition of the GHSI.
Beyond the GHSI
However, the impact of COVID-19 makes clear that we need to address factors that the JEE and GHSI do not measure and perhaps cannot measure. Institutional knowledge, a sense of urgency, relationships established in living memory, cross-sectoral logistics and resilience, all these factors may be critical to responses, and difficult to measure.
Other overlooked factors may include: root cause analysis of laboratory accidents and near misses; gathering intelligence on biological threats; cyber-biosecurity practices; the capability to strictly manage borders and quarantine; the elimination of wet markets and wildlife trade; and the apparent negative impact of sanctions, federalism, the politicisation of media and misinformation and disinformation on social and mainstream media.
Enhancing health security needs to be one of the world’s foremost projects (in the vein of climate action). This is for a number of reasons:
The rising risk of accidental bioengineering disaster
The rising risk of powerful biological weapons
The rising risk of AI enhanced biological manipulations
The likelihood of future pandemics
The clear inadequacy of the present IHR to ensure protection
The obvious cost-effectiveness of preventing biological catastrophe
How Much Will it Cost?
The cost of bringing all countries up to a minimum level of health security is probably marginal in the context of COVID-19. We found some evidence that that the US investment of a mere $1 billion correlated with significantly higher GHSI scores on average across 31 countries (+6 points overall, +10 for detection & reporting). For context, $1b is only 1/2000th of the initial US Congress COVID-19 stimulus package. The WHO has estimated it would cost $100 billion to bring 67 developing countries up to IHR compliance. Given the stakes (trillions lost to COVID-19) this is a no brainer.
The Path Forward
More will need to be done, especially in light of COVID-19, including structural changes to the IHR, and the process by which WHO declares PHEICs. Developed countries should increase their overseas development assistance to the 0.7% of GDP recommended by the UN and target their own gaps in health security. Many critics have suggested paths forward, see the following links for examples:
At the time the world had never heard of a company called Cambridge Analytica nor had any inkling of SARS-CoV-2. Unknown to me, at that exact time, Jaron Lanier was writing a (much better than my talk!) book about the malignant impact of social media on our wellbeing and society. It was called ‘10 Arguments for Deleting Your Social Media Accounts Right Now’ (Note, Lanier is not the titular asshole of this story).
After dabbling in the philosophy of AI, I returned to pandemic threats, publishing a blog in November 2019. Right when a bat was infecting the first Wuhan citizen with SARS-CoV-2, the blog provided commentary on the Global Health Security Index (GHSI), an index that conveyed a grim assessment of pandemic preparedness around the world.
In the present blog, I want to draw these disparate and seemingly unrelated related strands together. My thesis is that the business model of social media has played a critical causal role in the deaths of probably hundreds of thousands of people due to COVID-19.
‘Delete your social media right now’
Lanier was an early virtual reality developer, and has been involved with Internet2, Google (which bought his company), Second Life, LinkedIn, and a host of other digital projects. He is also a classical composer. He argued in his 2018 book that we would all be better off deleting all our social media accounts ‘right now’ and he has no social media himself at all.
In his entertaining yet serious way Lanier describes the business model of many social media platforms as: ‘Behaviors of Users Modified, and Made into an Empire for Rent’, aka BUMMER.
As we have come to understand, the social media platforms effectively sell users attention to advertisers (Lanier says ‘manipulators’) and the platforms deploy ever evolving algorithms that serve up content shown to enhance ‘engagement’.
The algorithm
What was not foreseen, but is now well understood, is that the algorithms soon learned that serving up individually tailored, controversial, emotional and negative content not only enhanced engagement, but turned us all into self-obsessed assholes, at the same time undermining truth, empathy and happiness (among other things). The details of all this can be found in Lanier’s book. Furthermore, it was not only this Unforeseen Disaster that has led to these problems, we also see Gaming the System on the part of content creators (eg Media hacks) and subversive elements (eg Russian trolls)
Lanier’s arguments for deleting all social media boil down to the following list of negative effects that the BUMMER business model has on individuals and society.
We’re losing free will
We must resist the insanity of our times
We’re becoming assholes
We’re losing truth
What we say is becoming meaningless
We’re losing our empathy
We’re becoming unhappy
We’re losing economic dignity
Politics is becoming impossible
We’re losing our special personhood
One example Lanier gives is the emergence of the Black Lives Matter movement (the first time around), which was facilitated by the internet and social media. So far so good. But then the algorithms determined that there was a subgroup of white, right-leaning, American nationalists who engaged tremendously with the platform whenever they were served BLM content. No doubt this is how future civil wars begin.
Lanier even gives the example of social media’s causal role in the malignant growth of the antivax movement. A perverse effect of the BUMMER algorithms is not only do they serve up antivax material because it pushes the right (or wrong!) buttons for various people, but then online marketplaces like Amazon will serve up antivax book suggestions because the user has been reading antivax material! This digital perpetual engine drives resoundingly crackpot content onto the bestseller list. Lanier puts it plainly in ’10 Arguments’ when he states that ‘BUMMER kills’. It literally does.
Which brings us to COVID-19.
The asshole
Donald Trump (the asshole of this story), having evolved into even more of an asshole through his literal addiction to Twitter and its empathy destroying asshole-o-genic psychological impacts, proceeded to divide the United States (and therefore the world) on almost every issue to do with COVID-19. Amplification of this messaging by social media algorithms, which served each item to those most likely to be pissed off by it, and by media outlets who created content most likely to piss everyone off (they know how they algorithms work and want their hits), consolidated the in-group/out-group psychology of left and right. Suddenly, a million people are dead worldwide in part because angry Trumpers (or Bolsonaros, or ‘Sovereign Individual’ Australians) won’t wear masks or stay home (nor sacrifice anything of relatively minor import in the interests of public health).
Remember the GHSI, I mentioned at the outset, used for scoring health security? Well the USA topped the index with 83.5/100. Ironic, I know.
The virus
In an article published by Sawyer Crosby (and others) on the ‘Think Global Health’ website, the authors ridicule the GHSI. They basically argue that we clearly have no understanding of how to measure health security if there is demonstrably no correlation between GHSI scores and COVID-19 outcomes (in fact, as at 31 July 2020, there was a correlation, and the GHSI was positively correlated with COVID-19 death per capita – at first glance it literally couldn’t get much worse for valid measurement).
However, any attempt to rank COVID-19 responses is surely premature. In the first instance, we don’t actually know how many cases there are globally (we do know there are at least 5 million in the USA!) An MIT study indicates that there are probably more than 100 million cases worldwide. This means that present estimates such as those compiled by worldometer are out by an order of magnitude due to undercount. Many countries are simply unable to count their cases as noted by this article in the Guardian. The flip side of a low GHSI score is that the country most likely has a low capacity for situation awareness as the pandemic hits (hence reports ‘low cases’).
However, I reiterate, we know for sure that nearly 200,000 US citizens have died. Other reasons why we can’t yet know which countries are doing well include:
COVID-19 ‘success’ will depend on the strategy chosen by each country (eg, exclusion, elimination, suppression, or mitigation)
countries impacted later can learn from those impacted earlier
the pandemic is still accelerating
countries that have done well so far may yet be overwhelmed
countries performing ‘poorly’ at one point in time may yet look successful in the future, eg, if they develop vaccines and roll out vaccination quickly
So, do we know how to measure (and therefore construct) global health security? Yes. But building the boat and sewing the sails and taming the wind will not get us anywhere if social media is telling people to jump overboard.
Let me be clear. No one invented social media with the intent of throwing people overboard, but the interaction of the algorithms, the assholes and the virus have almost certainly amplified the number of deaths in the United States and likely elsewhere. And those with an interest in a weakened USA are likely fanning the flames. We don’t know yet if the literal attacks on public health professionals in the US, as described in the Journal of the American Medical Association, were incited by domestic division, or Russian bot armies.
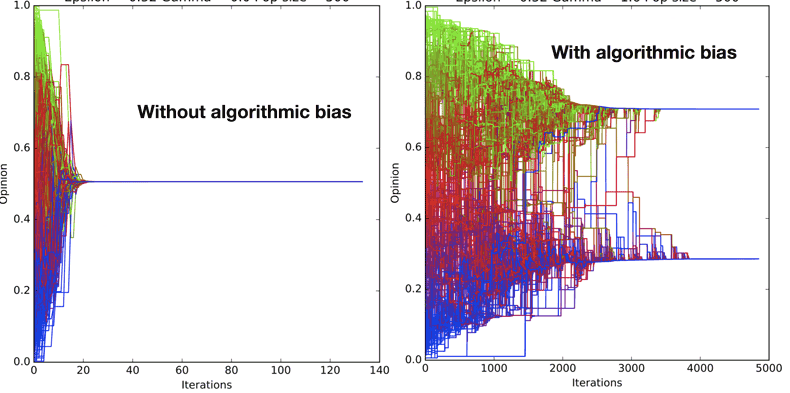
The USA should have been the country best positioned to deal with COVID-19 effectively and safely. Yet social media platforms have hijacked our cognitive biases, produced a general decline in civility in political discourse, and hardened value conflicts. Look at this figure which contrasts a simulation where a group of people with disparate opinions interact (on the left) to form an agreed opinion, with a simulation (on the right) where algorithmic bias feeds content similar to already held beliefs to the individuals. The result in the presence of algorithmic bias, is a persisting dichotomy of opinion (study available here).
We know that people follow public health guidance when they believe that officials understand the public’s values and that ‘people like me’ can help make decisions. When everyone scrolls through a highly individualised social media feed, there is no such thing as ‘people like me’.
In attempting to attain health security we have not adequately accounted for social media and the machinations of BUMMER. We did not consider that people might drink bleach because the president suggested so. We have tried to include measures of ‘political stability’ in the calculus of health security, but we did not consider the supreme assholery of ‘sovereign individuals’.
The future
In the big picture, COVID-19 is minor blip. The world will go on. But if there ever was a truly existential threat, a devastating bioweapon unleashed across the globe that required everyone to take action to ensure planetary safety, then under the current regimen we are screwed. We need a mechanism for coordinating or it will be the end of us. BUMMER must end. Health security must demand it. We need a period of wisdom and coordination to prepare for the greatest of threats. The alternative is that social media explains the Fermi Paradox.
In this paper (which I co-author), we argue that New Zealand’s health outcome appears to be the best in the OECD, but that some other countries made better use of certain control strategies. For example, Taiwan avoided an intense lockdown by focussing more strongly on immediate and intensive border control measures. Taiwan also excelled at using digital contact tracing and widespread use of face masks.
We suggest that in the post-pandemic era there are many emerging opportunities for society to be gained by embedding better plans for controlling future emerging diseases, and strengthening public health infrastructure.
Moving forward there is an opportunity to embed other important changes such as a ‘green reset’ and other pro-equity health interventions in system changes that will naturally follow the COVID-19 pandemic.
Growing mushrooms: just one way to protect humanity in a period of reduced sunlight
“Governments routinely ignore seemingly far-out risks. Rocked by a global pandemic, they need to up their game” (The Economist, 27 June 2020).
It is not clear whether risks that threaten human extinction have received appropriate attention at the level of international governance. We systematically searched the documents of the UN Digital Library and concluded that they have not. Our results and commentary were recently published in the international journal Risk Analysis. In this blog we give an overview of existential risks, our findings and possible international and national solutions.
Existential risks
The COVID-19 pandemic is clearly a very serious global disaster, but there are threats much more dire than COVID-19. These include threats that have a long history of international attention, such as a US-Russia nuclear war, and also those that are new or less familiar such as technological risks including geoengineering or synthetic biology. In the extreme some large-scale global catastrophes could threaten human extinction. The following is a list of some plausible threats to human survival:
Nuclear winter (the sun is obscured by soot from burning cities following a nuclear war)
Artificial intelligence (AI; machines are developed in the future with goals that are not aligned to those of humanity and wreak havoc)
Synthetic biology (engineering principles are used to produce dangerous biotechnology, including devastating bioweapons)
Geoengineering (modification of the atmosphere or oceans to mitigate climate change goes wrong)
Nanotechnology (nano-scale engineering creates a runaway process that degrades the environment)
Asteroid/comet impacts (a large object(s) collides with the Earth causing mass extinction as with the dinosaurs)
Supervolcanic eruption (massive volcanic eruption causes a decades long drop in Earth’s temperature)
Experimental physics disaster (high-energy physics experiment creates a devastating physical process such as a black hole)
This list of existential risks is not exhaustive and others include: risks of catastrophe due to biodiversity loss, ecosystem collapse, societal collapse, solar storm, a flood basalt event, a close supernova/gamma-ray burst/magnetar explosion, or even attracting the attention of harmful extra-terrestrial intelligence. There are also as yet unknown risks.
Many of these threats are not stand-alone threats but could combine with other risks. We can imagine scenarios where AI is deployed to aid the development of dangerous biotechnology, or where a pandemic emerges in a period of low health security following a nuclear war or comet impact.
Active mitigation of extinction threats is justified by the perspective of long-termism, which is grounded in the vast expected value of future human lives and the common desire to preserve aspects of the “human project,” such as our intergenerational cultural, scientific, and technological endeavours.
Results from our analysis of the UN Digital Library
We examined the UN Digital Library for evidence of any general international discussion about risks that threaten human extinction and also for evidence of discussion of the eight specific existential threats listed above.
Our search for 22 synonyms of existential risk in the UN Digital Library returned 97 relevant mentions. Over two-thirds (69%) of these pertained to nuclear war. Climate change was the threat mentioned 24 times, however in these cases the context was often an existential threat to island states rather than humanity as a whole. There were a handful of references to existential threats in the context of general disarmament or weapons of mass destruction.
Strikingly, searches of the UN Digital Library revealed few if any other categories of existential risk raised in a manner that made the threat of human extinction salient.
UN documents that explicitly discuss human extinction have a limited focus
On the basis of the keyword search it appears that the UN has a long history of addressing the threat of nuclear war and has engaged with the threat from comets and near-Earth objects through the Committee for the Peaceful Uses of Outer Space. These results seem to indicate a lack of attention paid to most existential risks.
Why is there little attention to existential risks?
There are clearly competing demands on national and international policymakers. Immediate threats such as regional conflict, trade, poverty, local health and education issues, as well as environmental concerns, weigh heavily and cannot be ignored. Yet the COVID-19 pandemic has demonstrated the economic and human devastation that arises if low probability or infrequent but catastrophic hazards are ignored.
Mitigation of existential risk is a global public good. We’ve seen with climate change how large-scale cooperation is needed to counteract the tendency for markets to undersupply such goods.
It is also the case that international policymakers are not well acquainted with considering human extinction. Theory and frameworks may be necessary to facilitate the right discussions. However, classification frameworks for severe global catastrophic risk scenarios now exist and can aid in exploring the interplay between many interacting critical systems.
Us humans are also subject to psychological biases that may prevent action. Time discounting means that we tend to prefer value now to in the future. This is unfortunate for future people and the intergenerational nature of the benefits of existential risk mitigation. Future people perhaps stand to benefit most, yet they lack a voice in present policy decisions. This needs to change and the rights of future generations could be enshrined in the universal declaration of human rights.
The very fact that humanity has not yet gone extinct might also lead to neglect of extinction threats. However, this would be a mistake. We may just have been lucky to date, and changes to our situation including new technological developments can shift the odds.
Some existential risks are new (such as AI and synthetic biology) and it may take time for them to filter through to political discussions. However, given the potentially long time-lag from substantial and wide-ranging discussion to effective mitigation, this does not mean that attention can be deferred.
International solutions
Early research on existential risks focused on the kinds of threats listed above as isolated exogenous events. However, these hazards cause harm because human societies are vulnerable to harm. Also, large scale risks are inextricably linked to governance failures, they are not merely challenges for governments to overcome. It is not clear that we are developing, deploying, or governing our technology with enough wisdom. This means that as well as implementing safeguards, we should also expect safety systems to fail and have a backup plan to mitigate the impact and survive these catastrophes if prevention fails (see below).
We are right to continue to be very concerned about nuclear war and major asteroid/comet impacts and should try much harder to prevent them. However, major Earth-impacts (although able to strike at any time) are extremely low probability events. Therefore, we ought to be more concerned over perhaps a five- to ten-year period, with developments in synthetic biology and AI. The power of these technologies is advancing rapidly, and we may need important norms and international regulations to prevent dangerous use by states, institutions or individuals.
There are four obvious things that member nations could lobby the UN to do:
Ensure that relevant bodies exist at the UN, similar to the UN Office for Disarmament Affairs (nuclear weapons), or the Committee for the Peaceful Uses of Outer Space (asteroid/comet impacts), to study and effect mitigation, and to coordinate the response to each specific risk.
Ensure there is an overarching bodyon existential risk across these committees that addresses existential risk as a category and focuses on vulnerabilities and resilience, rather than any single particular risks. This is important because the probability, magnitude and tractability of each threat vary, and resource allocation must be prioritised. By taking an approach across a portfolio of risks, and working on quantitative risk assessments, which account for hazards and vulnerabilities, this body would then be able to recommend which risks justify greater or lesser immediate resources.
Enshrine the rights of future generations: the UN Human Rights Council might consider options for approaching the rights of future generations. Any such rights, should they be deemed relevant and possibly enshrined in the UN Declaration of Human Rights, could have a significant effect in guiding mitigation action across UN member nations.
Develop a convention against omnicide, and any technology that could facilitate omnicide (such as possession of more than 100 nuclear weapons, possession of particular types of bioweapons, development of environmentally devouring nanomaterials, human germline manipulations causing sterilization, and so on).
National solutions
Given the immense consequences of existential threats, international governance should clearly expend some resources to study how to prevent and mitigate these threats. However, organisations such as the UN arguably have a chequered record of responding to crises. Also, some existential threats may not require a global response. Therefore, national governments, communities and individuals should all do what they can to help mitigate the threat (eg, the US Government unilaterally invests in asteroid detection).
At the level of national government, dedicated departments can study and monitor a portfolio of catastrophic risk, allocating resources to those threats with the largest expected impact (on the basis of probability, magnitude, tractability and neglectedness). In February 2020 we published a paper on AI that discusses this approach, in the context of New Zealand.
Prevention, resilience and recovery
Government action should address prevention, resilience and recovery. Prevention might include multilateral disarmament negotiations, revisions to the International Health Regulations to ensure the world is prepared for a catastrophic pandemic, and regulation and oversight to ensure the safety of technologies such as AI, nanotechnology, geoengineering, and synthetic biology. Prevention might require very rapid action at the time of catastrophe. With COVID-19, New Zealand had the luxury of learning from other nations and imposed border controls just in time. Future catastrophe could strike a country like New Zealand first, and so rehearsal, simulation, and walk throughs of key actions are needed ahead of time.
Resilience could include economic preparedness. In the case of New Zealand, the Earthquake Commission model could be enhanced and extended to all catastrophic threats. An investment of 0.5% of GDP per annum could provide in the order of NZ$100 billion per generation to deal with unprecedented catastrophe and could have been accessed for the COVID-19 recovery. Pandemic reinsurance products briefly existed. These married superannuation funds (which save on pay-outs when there is a lot of death) with businesses (which suffer losses during pandemics). However, these no-brainer products were not popular with businesses that clearly felt pandemic insurance was not needed – but such thinking may now be changing. Many other creative ways to fund catastrophe may exist.
Resilience can also be built at the level of individuals, communities, and local governments. Researching and implementing strategies to help individuals and towns ensure food production in a world with a period of reduced sunlight would provide resilience against nuclear winter, supervolcanic eruption and asteroid/comet impact.
Recovery might hinge on some region or population avoiding a global catastrophe and being well-positioned to re-seed the Earth with people, technology and know-how. Partitioning the population to escape a catastrophic pandemic or facilitating survival in islands geographically most likely to endure a period of reduced sunlight could help. International law might need to be addressed. For example, the International Health Regulations actively deter restrictions to travel and trade to combat pandemic disease. This may need to change to empower island nations to close their borders and provide a reservoir of human capital and technological know-how to rebuild civilisation after a catastrophe.
Summary
Existential risks appear neglected by international governance. COVID-19 shows that we must invest time and resources to understand large scale risks. We must also begin preparations to mitigate the most general effects of these threats. This includes implementing appropriate oversight and safety engineering of potentially dangerous technology, building resilience to survive a world with a period of reduced sunlight, and planning to partition humanity so that risks cannot spread to every last grouping of humans.
We risk being limited by our naïvety of many complex processes and may require new methodology and cross-disciplinary work to evaluate these threats. Governments would do well to begin by bringing the full range of domain experts to the table.
A new paper explains how the GHSI can be used to guide preparations in New Zealand and the Pacific
New Zealand has done well to date in managing and eliminating (for now) COVID-19 disease. However, there have been sensible calls for an inquiry into New Zealand’s response. An inquiry could help determine what worked and what didn’t, what went well, and how we could do better next time. An inquiry should focus on ways to get the same result while suffering less harm (economically, socially, and in terms of health).
The Global Health Security Index
Fortunately, there is a lot of guidance for planning, such as The Global Health Security Index, which in 2019 independently scored countries on 140 items relevant to health security (NZ scored 54/100). This index highlights the diverse factors that go into protecting health by preventing, detecting, and responding to a threat, as well as the robust health system, commitments to international norms, and a well-managed risk environment that reduce the chance of harm.
Work should begin now to determine how the GHSI can help to prevent and manage the next threat. A paper published today (12 June 2020) in the New Zealand Medical Journal does exactly this, by explaining how the new GSHI can help guide New Zealand’s planning for biological threats, and also help enhance Pacific regional health security.
Improving preparations for biological threats
The paper on GHSI published today describes NZ’s score, as well as those of our Pacific neighbours. It outlines how New Zealand might better prepare and improve its resilience against the next threat. It also explains why aiding Pacific nations to enhance regional health security is critical. Given the potential for rapid spread of disease, if some are not prepared then no one is fully prepared.
The risks of anthropogenic threats (lab accidents, malicious use of biological weapons) is high, and the damage from these could be vast. Fortunately, there are many other tools in the GHSI toolkit that ought to be implemented now, to prevent accidental, unforeseen, unprecedented, or malicious risks before they occur.
These include screening of all DNA synthesised to order, consolidation of dangerous materials in a minimum number of laboratories, and standardised biosafety and biosecurity training. We also need a plan to protect vulnerable populations, such as residents in aged care facilities.
We need a generic pandemic plan, fit for all purposes, that is not merely based on pandemic influenza and a ‘let it in and manage it’ approach. Beyond pandemic planning however, there is much that can be done to reduce future biological risk. COVID-19 was nothing like influenza and the next threat could be nothing like COVID-19. Imagination is needed.
Border closures
Perhaps most critically, we need to better understand the criteria for border closure and border management mechanisms. Repeatedly over the last 3 years, prior to COVID-19, the Ministry of Health had been adamant that border closure would never be used. And yet, the first thing that New Zealand (and many other nations) did in the face of the COVID-19 pandemic was to start to close, and then completely close, the border.
It is entirely possible that the economically crippling level 4 lock-down might have been avoided with well-planned, well-rehearsed, early border closure according to pre-determined criteria. More thinking about when to implement border closures is needed.
Beyond GHSI
But we must also think beyond the GHSI because no single tool anticipates everything, and recent events (in NZ and around the world) demonstrate the importance of managing misinformation and disinformation campaigns, of avoiding the politicisation of public health emergencies, of quick decisive action, and of equitable and universal access to healthcare. There is much more that we can do to preserve human health in New Zealand and regionally in the face of inevitable future biological threats.
Following a recent post on the University of Otago’s Public Health Expert blog, Matt from Adapt Research discusses COVID-19 with Radio New Zealand’s ‘The Panel’
The only way to contain coronavirus cases in NZ is to go to Alert Level 4 for a brief period.
New Zealand currently has an unknown number of coronavirus cases wandering around our community. A number of observations support this, first is the experience of many other countries, second is the sudden growth in confirmed cases, third is that we have a cohort of international arrivals (and returning New Zealanders) who came to NZ between March 5-15th. This means they arrived before the mandatory 14-day quarantine, but still within the virus incubation period. Virtually all our new cases are from this cohort.
We now have a 4-level alert system. This is an excellent tool to get everyone on the same page and clearly to communicate both risk and required actions.
We should be at Level 4 right now.
This would allow us to reduce to Level 3 and then Level 2 as quickly as possible and avoid protracted disruption. I will explain.
The target we are chasing is invisible and our confirmed data is always behind the brute facts of the situation. In a situation like this the ONLY strategy that can succeed is to draw the circle of containment as wide as possible and then move inwards. This means setting Alert Level 4 right now, stay at home.
Over the next 12 or so days, ALL the coronavirus cases would then reveal themselves with symptoms developing (or if it is a mild case the infection passing almost unnoticed) without infecting anyone else. Once we have identified ALL the cases, then they go into isolation and we have stopped the spread.
After two weeks, towns, cities or regions with no cases revealed can be set back to Level 3 and even Level 2 and business can carry on. Towns or regions with cases might hold Level 4 for another week. But everyone can very quickly get back to Level 2.
We can then release the strict controls and just deal with one case at a time as they crop up, all of which (theoretically by that point) will be cases of returning New Zealanders who will reveal their symptoms while in 14-day self-quarantine and this will not be problematic.
We then implement widespread temperature checks, hand washing, stigmatization of coughing etc. But business can carry on.
What this implies
Whether Winston Peters’ encouraging of New Zealanders overseas to return is helping or facilitating the problem. Places like Wuhan now look relatively safe. As long as people don’t transit through airports where they could catch the virus, there are many places that might be safer than attempting to return, and the likelihood of bringing disease back into a quarantine zone.
In the future when we get warning of a novel outbreak we ought to immediately and dramatically close down the world for 2-3 weeks for exactly the reasons that I’ve outlined above. This should have happened around Jan 20th. Previous times that we might have taken this approach would have been with SARS, Ebola, MERS, and now Coronavirus. This is about 4 times per 20 years, or about 20 times per century. It is far preferable to suffer 2 weeks of GDP losses twenty times than 18 months once. This is a no brainer, but the mechanisms need to be coordinated ahead of time. A 20:1 false positive rate needs to be seen as acceptable.
Hopefully, New Zealand decision makers see the logic in this and raise us to Level 4 today, for a period of 2 weeks to minimise our losses.
New Zealand has just shut its borders to foreign visitors for the first time in history in an attempt to mitigate the impact of COVID-19. In what follows, I outline the case for border closure, the conditions under which it is rational, and then note that this is merely one measure against one catastrophe. Moving forward, we should get used to analysing and preparing responses to such large-scale risks.
Closing the border in a pandemic
Pandemics impose costs on society. These costs include up front hospital costs, ICU costs, lost productivity due to illness, and death, and downstream costs including human and emotional toll and long-term productivity loss.
Closing the border also imposes costs, these include disruption, visitor revenue forgone and more than likely reductions in trade and business downturn. But importantly, closing the border can also fail, if a significant amount of disease gets into the country anyway (eg from returning kiwis), and if there is a substantial outbreak despite border closure then the costs of closure and the costs of the pandemic are incurred.
Keep the border open in a pandemic or keep the border closed, it’s a lose-lose situation. However, previous research has demonstrated that provided a pandemic is serious enough, meaning that a sufficiently large proportion of the population are likely to get sick (say, 40%) and the disease has a sufficiently high case fatality (say, very much worse than Spanish flu of 1918) then the costs of border closure pale in comparison to the costs of the pandemic. Border closure is then a no brainer.
Border ‘filtering’ and border ‘closure’
But there is border closure and then there is border closure. The current New Zealand policy, let’s call it ‘filtering at the border’, allows for the free passage of returning New Zealanders, provided they agree to pass through the ‘airlock’ of 14 day quarantine, and also allows for New Zealanders to leave and then return again (although this is advised against). Both processes could bring disease into the country. A policy of ‘complete’ as opposed to ‘filtered’ border closure would prohibit the movement of kiwis too.
Would ‘complete’ border closure ever be justified. Possibly yes. Imagine if the case fatality rate of COVID-19 was 100% instead of 1%. There could really be no justification for risking anyone entering the country at all until the pandemic was over. If such a case ever arose, then immediately sealing the border and becoming a ‘refuge’ is a completely rational approach.
But back to ‘filtered’ closure. The hope is that by filtering out foreign arrivals, then the impact of COVID-19 will be much less. This could still prove fruitless, either if there is established community transmission from the cases already here, or if returning kiwis bring the virus home and spread it. In our previous research we modelled a scenario where border closure is attempted but fails, resulting in 90% of the unmitigated case-load. For a pandemic of more than 10 times the severity of Spanish flu, this was still a cost-effective measure (minimizing losses) under some assumptions. However, for swine flu (2009) it was never cost-effective to close the border.
How bad is COVID-19?
COVID-19 is an intermediate case. Under the ‘base case’ model of 40% infected, half being asymptomatic and 1% case fatality for the rest, it could cause 1 million symptomatic cases, and 10,000 or more deaths in New Zealand. This is a huge human, social and economic burden with ramifications for our economy for many years. But these costs (the economic ones) only barely balance out the lost visitor revenue from say 6 months of border closure. So, at first glance the case for closure is equivocal.
If trade continues, though curtailed by a policy of border closure, then the numbers become important. If closing the border (successfully) means the pandemic costs you $11 billion less than it would have otherwise (which is the result of modelling 72% infected and 2.3% dying, hospital costs, productivity loss, death, etc), then it is worth closing the border even if there is going to be an $11 billion drop in trade over the period of border closure (about 20% of trade for a six month period).
What is hard to predict, but is becoming clearer, is the global impact of the pandemic on travel and trade. If tourism drops to zero despite our actions, and trade plummets too, then the economic benefits of closure compared to no closure, suddenly appear much greater. You lose nothing by closing the border if there is no tourism and no trade anyway.
These are the numbers that need to be evaluated for a range of scenarios. And on the basis of these numbers COVID-19 looks to be right in the middle, between swine flu and disaster.
This means the decision may come down to factors other than strict economic ones and three factors play a key role: equity, access to care, and the value of a ‘quality adjusted life year’ (basically one year of good health).
Equity, access and value of life
COVID-19 differentially impacts the elderly. They suffer more severe illness on average and bear the brunt of deaths. This may also be true of other minority groups in New Zealand, we don’t know this yet. Our health system places a lot of weight on equitable treatment and prioritising ventilators is not equity. The best strategy to make sure everyone has a fair chance might be to simply close the border and keep it out.
COVID-19 places an immense burden on critical care facilities, and our modelling suggests that with an infinite supply of ICU beds COVID patients could occupy enough of them to cost the health system $1.9 billion or more. However, we only have enough beds that $270 million worth could ever be continuously in use over a six-month period. So, the analysis suggests costs well in excess of those that would be realised (ie the outbreak seems to get cheaper). But this results in unmet health need. And likely would result in preventable deaths. Which have a long-term cost themselves. Again, these are the factors on the scales that need to be weighed.
The modelling research we did used Treasury figures for the value of a year of good health, which are derived from Pharmac funding decisions. Basically, how much does Pharmac spend on medicines that lead to a gain in one year of good healthy life?
It may be that we New Zealanders decide to put much more value on healthy life than this (double? triple? it can’t be infinite or there would never be such a thing as a health budget, it would be a blank cheque). But this new valuation, if imputed in the models, can change the outcome of these economic analyses.
So, closing the border to protect vulnerable populations, to ensure fair access to care, or to save lives can be a very reasonable decision, even when it is not strictly an economically rational one.
Border closure can still fail
Bear in mind that border closure could still fail and the probability of failure should be built into economic modelling. We could still end up with just as many cases as in the no closure scenario. Many other variables in this equation (such as the exact epidemiological parameters of COVID-19 in certain contexts) also remain unknown.
Given the high degree of uncertainty, it may be rational to close the border to assess the situation. This is because, although borders can be re-opened at a later date (even re-opened almost immediately), we may lose the window of opportunity to close them if we don’t act now. This decision and the precise timing are very difficult, and although detrimental economically, it may be wise to move fast, as the government has in fact done.
But now we risk a very long waiting game. The virus is likely to be controlled in some regions of the world and not in others, resulting in a patchwork of ‘hot’ and ‘cold’ zones and severe travel disruption until a vaccine is available. There is almost a paradox in being too successful. If we keep it out then we must sustain our vigilance for the long haul or risk an outbreak every bit as bad as it can be, just down the track.
Global Catastrophic Risks
COVID-19 is a very harmful event, but it is not a global catastrophic threat. There are worse scenarios waiting in the shadows, and we must be prepared for them. Our experience with COVID-19 and the substantial fall-out will hopefully now prime decision makers to be receptive to the idea of building resilience against catastrophic risk. There are far more devastating biological threats that could arise, whether naturally or through biological manipulation, there are threats from other technologies, such as artificial intelligence (AI), geo-engineering, nuclear technologies, as well as threats from climate change, supervolcanoes, near earth objects, and others. COVID-19 has shown us how fragile our just-in-time systems are, how pursuit of a point of extra return can leave us undercapitalised, without cash flow, without inventory, at the mercy of global forces.
The government ought to take a risk portfolio approach to global catastrophic threats, and invest in assessing the probability of various risks, their magnitude and how to build resilience against them.
There is no reason why we can’t have an EQC-style fund to protect against risks that hit only once per generation, but hit hard. There is no reason why we couldn’t have walked through scenarios like COVID-19 with all sectors collaborating to identify the bottlenecks such as ventilator availability, testing locations, health workforce, data systems to track those in quarantine and so on.
The current event involves a biological virus, what if the next event involves a digital threat, would we close our internet borders? What is the case for doing so or for not doing so? This all needs to be scenario-ized.
The first significant step is to institutionalise the learnings from COVID-19, the phrase ‘global catastrophic risk’, and a commitment to undertake research, analysis, planning and systems testing much more often and more robustly.