“COVID-19 has shown that assumptions about disease emergence and transmission and capabilities to respond to infectious disease threats are not only incorrect but pose a risk to global health security.”
A new article in the Lancet (8 November 2021) provides a peer-reviewed chronological analysis of crucial junctures and international obligations in the early days of the COVID-19 pandemic.
What happened day by day, where, why, or why not?
The information was gathered by the Independent Panel for Pandemic Preparedness and Response. The Panel was co-chaired by former New Zealand Prime Minister the Rt Hon. Helen Clark, and Her Excellency Ellen Johnson Sirleaf, former President of Liberia.
The following post blends the findings of this report with my interpretation of the early response to (future) pandemic-threatening outbreaks.
The article provides the following timeline of Covid-19 emergence (much more detail can be found in the Lancet article):
November 2019: human to human transmission was probably occurring in China (later evidenced by phylogenetic studies and epidemic growth rates)
8 Dec 2019: a patient is symptomatic with atypical pneumonia in a Wuhan hospital
24 Dec 2019: the patient’s lung fluid sent to a private laboratory in Guangzhou
26 Dec 2019: a woman with fever and cough in Wuhan has a chest CT suggesting pneumonia of unknown origin
27 Dec 2019: the woman’s husband and son have the same findings
‘Late’ 2019: possible spread of virus outside of China (weak evidence from heterogeneous unverified studies)
30 Dec 2019: Wuhan Municipal Health Commission issues first notices to hospitals with instructions not to share!
31 Dec 2019: Finance Sina reports the story, a machine translated version of the story is published on an emerging diseases monitoring website and picked up by the WHO.
31 Dec 2019: Taiwan and Hong Kong begin preparing interventions and screening travellers from Wuhan.
31 Dec 2019: Wuhan Municipal Health Commission issues a public bulletin describing 27 cases of pneumonia of unknown origin (not sent to WHO!)
5 Jan 2020: WHO notifies all country governments
5–7 Jan 2020: Multiple sequences of viral genome completed
8 Jan 2020: Case detected in Thailand by airport screening
10 Jan 2020: PCR test for virus developed
11 Jan 2020: PCR test for virus deployed
14 Jan 2020: WHO tweet states there is ‘no clear evidence of person-to-person transmission… but “possible”’
20 Jan 2020: confirmed human-to-human transmission (health workers infected)
22 Jan 2020: WHO International Health Regulations (IHR) emergency committee convened
23 Jan 2020: 581 cases confirmed including 10 outside of China
23 Jan 2020: Strict public health measures in Wuhan (retrospective analysis indicates that 86% of cases were undetected at this point)
24 Jan 2020: WHO recommends against travel restrictions
30 Jan 2020: Public Health Emergency of International Concern (PHEIC) declared by WHO Emergency Committee but travel restrictions recommended against, WHO director general states we must ‘protect weaker health systems’ (this perhaps implied that ‘stronger’ ones might not need to prepare much)
Computational models predict virus spread along air traffic routes (which could have allowed mass targeted surveillance testing)
11 March 2020: the word ‘pandemic’ is used by the WHO Director General
11 March 2020: First European country (Italy) enacts national lockdown
An interpretation of this timeline
My interpretation of this timeline goes something like this:
Given the extreme global threat of an out-of-control novel respiratory pathogen, in the future, cases like that admitted to a Wuhan hospital on 8 Dec 2019 should have samples taken immediately and any viruses isolated and sequenced. If the genome bears any remote similarity to respiratory pathogens of concern, then a public health emergency of international concern (or some similar alert) should be issued immediately (ie at least a month before it was for Covid-19).
The family cluster on Dec 27 is suggestive (though not proof of) human-to-human transmission. Given the extreme global threat of an out-of-control novel respiratory pathogen, in the future, human-to-human transmission should be assumed at this point, and the WHO informed. Given the retrospective analysis mentioned above, in the future, we must assume there are many more cases than data suggests at an early stage.
The question of whether the virus was spreading outside of China before 2020 is critically relevant. This is because strong public health measures can quash an outbreak like Covid-19 in its early stages, as measures in countries like Taiwan, New Zealand, Australia, and China have repeatedly shown. And with a limited number of identifiable outbreaks very strong initial measures would be justified to prevent a pandemic. However, with widespread and undetected escape of a virus like Covid-19 the argument for strong lockdowns is weakened.
Given the extreme global threat of an out-of-control novel respiratory pathogen, in the future, we should conduct very widespread and rapid initial testing worldwide (targeting transport hubs). In the future we must ensure:
A substantial supply of testing capacity (this will mean planning to develop and deploy a test at scale within days of outbreak notification)
Dispensing with ‘criteria’ for testing. With Covid-19 many probable cases were not tested because the criteria and case definitions targeted only travellers from Wuhan or those who had contact with travellers from Wuhan.
Speedy action is critical. As evidenced by the fact that Taiwan and Hong Kong had some of the best pandemic responses globally through 2020, and they acted weeks before the PHEIC was finally declared. Given the extreme global threat of an out-of-control novel respiratory pathogen, there is nothing stopping every country in the world acting at the same point in an outbreak (ie the equivalent of 31 December 2019 in the Covid-19 situation) and preferably earlier (as above).
In sum, it should be possible to identify a similar virus of concern at least 16 days earlier (testing on 8 Dec vs 24 Dec as above) and therefore prepare to act internationally on a date equivalent to 15 Dec 2019 (16 days before Taiwan and Hong Kong did). Extreme public health measures at the point of origin could then be enacted on the equivalent of Dec 27–30, when suspicion of human-to-human transmission emerges along with case series reports. This would be nearly a month earlier than Wuhan did in fact lockdown. This apparent ‘overreaction’ would be justified by the global health and financial impact in expectation, conditional on the finding of person-to-person spread of a SARS-like respiratory virus (see ‘cost effectiveness’ below).
Recommendations of the Independent Panel
On the basis of the timeline above the Independent Panel recommends reform of existing laws, governance systems, the IHR, and a pandemic treaty.
The Panel’s notes and recommendations include (a fuller discussion is found in the Lancet article):
That the IHR are less proactive and time-sensitive than is optimal in the face of a high-transmission respiratory pathogen.
Remove constraints on WHO reporting publicly prior to verification
Streamline the WHO verification process
Ensure open and transparent proceedings of the Emergency Committee
Presume assistance/cooperation of States Parties will be needed
There must be a ‘special urgency’ around coordinated, evidence-based, and international governance for zoonotic risk.
Rigorous translational activities, including the use of epidemic simulations that test capabilities, should be used to identify deficiencies to correct (this item seems particularly relevant to New Zealand given the general sense of playing catch up with public health capabilities even when future need is identified – had NZ simulated contact tracing 200 cases per day?)
Proactive global surveillance (not syndromic testing) when a respiratory pathogen suspected
Future outbreaks should be approached with a ‘rebuttable presumption’ of sustained human-to-human and asymptomatic transmission
Assume far wider spread than is evidenced by the data
Full and immediate reporting of any possible high-impact respiratory pathogen to WHO (through a process more expedient than the present IHR requires)
Full authority should be granted to WHO to investigate pathogens with cross-border potential
The WHO Emergency Committee should give greater weight to the potential costs of not declaring a PHEIC
A global pandemic treaty should be created centred on the principle of equity
Generally, much broader deployment of the precautionary principle
Cost-effectiveness
Some may question the cost-effectiveness of extreme initial public health measures, given the severe costs imposed by border closures and lockdowns. However, the cost-effectiveness must be seen at a global level. Extended and repeated extreme lockdowns implemented globally are clearly not cost-effective for a Covid-like virus (when using thresholds typical for health interventions, as a number of analyses have shown), but shorter lockdowns targeted to quash the outbreak in its early phases may well be highly desirable (when seen in a global context).
The total global cost of the Covid-19 pandemic is estimated to be well over US$20 trillion. Even if only 1 in 100 concerning outbreaks of respiratory pathogens with suspected human-to-human spread would in fact lead to a Covid-like pandemic, then it is rational to spend up to US$200 billion to ensure we stop each one. Some lockdowns in New Zealand were costing NZ$1 billion per week. Back of the envelope calculations therefore suggest the world could implement extreme public health measures for 6 weeks, across 30 or 40 locations of 5 million people to ensure strict control of an outbreak is obtained, and to do this on 100 separate occasions, and still be better off for it! The proof of concept is the success of even Wuhan’s (late) lockdown. Lesser measures might have worked if enacted a month sooner and simulations of spread via travel hubs points to where we should act.
However, given that the cost-effectiveness must be seen at a global level, there must be mechanisms enacted to ensure just and equitable impact across the world, so that regions that must necessarily undertake extreme public health measures to prevent a global pandemic are compensated for these measures. This is in the interests of all States and should be worked into the refreshed IHR.
However, the critical caveat is that strict public health measures will rapidly become cost ineffective if endlessly repeated during the same outbreak or continued for too long. We must take extreme measures initially but be prepared to rapidly reduce them if they fail. Some a priori public debate around cost-effectiveness of extreme measures, and in particular the value of life in pandemic situations is warranted.
Sometimes creative writing can be leveraged to trigger productive reflection on complex issues. This post includes the full-text of a short story on catastrophic risk, ‘The Sequence Matters’. It is an entry in the Effective Altruism Forum’s Creative Writing Contest.
Effective Altruism is a community that addresses issues such as existential risks to humanity, how to do the most good possible, and what the most rational global priorities are.
EA has been running its creative writing competition because stories have been a key factor driving EA’s growth since its inception. Influential stories include those by: Peter Singer, Eliezer Yudkowsky, and Nick Bostrom.
What follows is my entry in the EA Creative Writing Competition. I hope you enjoy it.
The Sequence Matters
(5000 words)
I
When a structure kills by collapse, investigators search for causes. Perhaps design was flawed. Perhaps maintenance neglected. Perhaps the wrong structure had been built in the first place.
Everton remembered interrogating C in prison. After obtaining his evidence, he chose to leave the heavy cell door unlocked. Clueless then to the consequences of his actions.
Lord Thomas boomed.
‘I cannot help but think, Mr. Everton, that our being here today poses many more questions than we seem to be answering.’
The Supreme Justice shifted on his throne. His every glance captivating onlookers in the gallery. The Justice eyed his peers at the bench, stroked his ample beard and tapped his pen. Pointing at Everton in the witness box he spoke again.
‘It’s clear that we congregate today due to the actions of someone known simply as ‘C’. And I cannot fathom why no one is able to tell me more about them than an initial. But what is even less clear, Mr. Everton, is the role that you played in what can only be described as the catastrophic events of six months past.’ Thomas paused and checked his papers.
‘C was a woman,’ said Everton.
‘What’s that?’ hissed Thomas.
‘I’m telling you more about her,’ said Everton. ‘C was a woman’.
Thomas carried on, ‘Furthermore, as Justice Parata has significantly brought to our attention, we must ask had this disaster never been predicted by the mysterious C, would it even have occurred at all. And if it weren’t to have occurred at all, would it have ever been predicted? You see the awkward position we all find ourselves in. Such are the questions that stalk our collective minds. And,’ Justice Thomas drew a breath, ‘We are well aware that C did not survive these events, so we have no recourse to an interrogation of… her. Indeed, it seems no key witnesses remain alive, except, mysteriously it must be said, for you Mr. Everton.’
‘C had a moral heart,’ said Everton. ‘But more than that she had a moral mind.’
‘It is not some disembodied mind that is on trial here Mr. Everton…,’ Thomas spoke with force.
‘And just who is on trial Jeremy?’ The gallery breathed a collective gasp as Everton addressed Justice Thomas in the familiar. ‘Who is on trial? The dock stands empty like some gaping sore.’
‘Mr. Everton, we don’t need a defendant to hold court. As we proceed the defendant will take shape. We seek justice in its purest form. Words easily bring that which does not yet exist to life. The papers will write about it and the defendant will be as real as you or I. As real as her alleged crimes, and as real as the Law itself.’
‘And the wound will ooze, responsibility will fade in phantoms.’
‘Mr. Everton, you walk a very fine line!’
‘You have no idea how fine that line is Jeremy. You have not heard what I have now heard, have you? That’s why I’m here today after all. I mean how could you have. When did you last leave these chambers? Ever since your appointment you have been preoccupied with your precedents and papers, nothing more. You are the prisoner here!’
The gallery gasped again.
‘I stand here wondering,’ Everton continued, ‘how all this came to pass. We sat side by side, you and I, the same lecture halls, the same exams, with the same ideals and hopes. But that was a long time ago, and now you sit there as Chief Justice and I stand pleading with you, offering truth after truth and you cannot hear me. What made you so different from me?
‘We are the ones asking the questions here. All you need do is answer,’ said Justice Thomas.
‘Don’t lecture me of all people on interrogation Jeremy. If it weren’t for my methods you wouldn’t even have chambers to preside over.’
‘Everton. What exactly is it that you believe we need to know? I am listening. Forget all this theatre. Explain it to me.’
‘I fear that some lessons seem simply unable to be learned. But I am willing to take you through the evidence. Step by step.’
As Everton began to relate the story, a small girl in the public gallery gripped her mother’s hand and a tear slid from the corner of her eye.
II
C opened her eyes. A scuttle of rats’ claws vanished in a corner. She turned on the light. She was sitting at her desk. She had dreamed of an open door and a masked face. Now she was awake, wide awake. The windowless room around her was sharp with detail, but unfamiliar, older somehow, or more distant. Her mind wandered far from the desk in front of her. C had not remembered falling asleep.
The tower is unstable, she thought. It’s going to collapse.
C rose from the desk. She felt grounded. Before she stepped toward the door she could see herself opening it. Her movements like a lagging image, but lagging forward.
The corridor was a swarm of construction. Panels missing, pipes and girders exposed. An organic lattice of curves and fractals. A welder focused solely on an incandescent arc.
When she got to Chad Schwartz’ office she already knew Schwartz wouldn’t understand. He’d repeat the mantra, the algorithm says it will work, the tower supports our flourishing.
‘Wait a moment,’ said Chad Schwartz holding up his hand at C’s entry. His attention and that of his aide was directed at a glass tank. In it a rat sat on a platform surrounded by water. The rat was gnawing on a stack of hard uncooked spaghetti. On another platform was a large stack of food, and the exit.
‘Wait for it…’ said Chad, ‘there!’
The rat was inching the last stick of spaghetti across the span between the two platforms. Sniffing the air, it took a nimble step onto the hard pasta. But the single pasta couldn’t support the weight. It snapped dumping the rat into the water.
Chad exploded in laughter, waved the aide away and turned to C.
‘There were times C, when your concerns were figured with pencil and paper. But the structure must expand, it’s our priority, and we have the algorithm now.
C said nothing. Dismissed before she’d begun. A glance at the letterhead of some paper in the trash as she departed. Schwartz Corp, with an inky black swan of a logo.
III
C returned to her office, clambering over cable spools and toolboxes in the hall. An arched ceiling reinforced with spidery piping. A worker unscrewing a railing, placing it in a carton of scavenged metal. Intent on a sheet of instructions.
C shooed a rat away from her desk and sat in the chair. The upholstery had been removed some time ago. Stalked by anxious thoughts of some distant disaster, she opened the book again.
C woke. The room around her seemed crisper than ever. Perfect contrast despite the low light. She felt herself drifting through hallways, climbing ladders, gazing to an unseen horizon, even as she sat in the chair.
The collapse could be soon, sudden, and sharp she thought.
She tried to decide if her mother would believe her. Or if it’d be like the time she’d found a dead rat in the kitchen drawer. She should’ve kept the stinky thing as evidence.
C began to write. She wrote about the problem of space, the uncertainty of the iron stack, the bottomless chasm, the bridge that had once been started, the reconfigurations of the tower, the doctrine of upward expansion, the calculations of balance and stability, she speculated about the outside, though she had never seen it. And these days she included the rats. With her new information, she projected forward, far forward.
She tried to sleep, occasionally a sudden sense of falling, halted by a gasp and the stutter of her heart. She wasn’t dreaming but everything looked different now.
She reached for the phone to dial her friend Nadia. But she quickly hung up. She wondered who might be listening.
The bulb of her desk lamp fizzled. The door to the office swung open. Silhouetted, a masked figure appraised her. Ten years working here she thought. This was something she had never predicted.
IV
‘This is so much more important than everything else,’ C said.
A strong breeze flowed through Nadia’s office. Nadia, focussed on the details of one of her origami birds, seemed not to notice. Black polythene fluttered against one wall. Rusted beams had been pushed through the wall into the office, realigning the structure’s skeleton.
‘Did you hear me?’ said C.
The figure in the mask shadowed her two steps behind. It had wordlessly followed her here.
‘Remember those jellies we shared as children,’ said Nadia without looking up. ‘Where was that, level twenty? The atrium balcony, I don’t remember the past so clearly.’
‘The level eighteen storeroom. Before it was sealed.’
‘Yes, that’s right. You stacked those paint buckets so high.’ Nadia laughed. ‘Oh the mess!’
C couldn’t help but laugh, ‘we should’ve taken our time, got the trolley first. Mum was furious.’
Nadia didn’t seem to notice the masked figure.
‘Anyway,’ Nadia said. ‘We have the algorithm now. One thousand elegant levels by the end of the year if you believe the forecasts. Which of course we must.’
‘But what about next year?’ said C. ‘Or a hundred years from now?’
‘Do you think this one’s pretty?’ said Nadia, still focused, and holding out an origami bird, ‘or should I start again?’
‘People will die,’ said C. She knew that was an understatement. But glancing at the masked figure she said no more.
V
C rode the elevator, traversing a cubic kilometre of the tower. The carriage now just a flimsy cage, its panels scavenged for the upper levels. Levels slid past in a blur. Rats clung to the exposed cables hitching a ride. The whole structure shuddered briefly.
C updated her prediction. The collapse was imminent.
She thought of Gustav and remembered a conversation they once had. The old man, her colleague, had been fussing over his coffee.
‘Gustav, I’m sorry, but I need to know about the rats,’ C had said.
‘No, no. None of that matters now, not like then, back then when we had a choice… I’ll tell you something else.’
‘Gustav this is important.’
‘Many things are important my dear. Your obligation to drink coffee with an old friend is important. Here, drink, focus on the moment. Most employees of this company have never taken leave you know. They have never stepped outside the levels of their offices and apartments, never sought to exit the tower, let alone seen the chasm. But why should they? What do they want for in here? Yes, there is a world beyond these walls. A world of endless resource. But people don’t covet what they know nothing of.’
‘Tell me about the rats Gustav. Have they always been here? Why doesn’t anyone control them?’
‘We used to suffer your structural failures, but they never amounted to much, we might expect similar threats in the future, but as we’ve learned they’re never an existential risk. Besides, we have the algorithm now and its precision is beautiful and flawless. You’ve seen the harmony of the girders we place. Structural stability is its primary goal, there is a counterbalance for everything.’
‘The rats Gustav.’
‘The bridge and the tower were under construction. We flourished, but we needed more space. We’d plundered the iron stack. But there was abundance in the half-finished bridge to repurpose. A structure stands on its core you see. So much else is unnecessary. Fractional reserve building. That was the great innovation. Decoration, furnishings, all repurposed as structural components. The tower continued to expand upon a foundation of clever calculations. And now with the algorithm, we’ve handed design to the machine. You’ve seen the forms it creates, organic designs, unfamiliar geometries. Beautiful, beyond our wildest dreams. Further and taller, and yet just as stable. Ten times the size of the original structure, by rearranging the same components. The algorithm showed us how to drill down you know. Deeper and deeper, expanding into the earth.’
‘Gustav I need to know about the rats.’
‘Yes, yes, I’m getting there. Patience. All these activities create risk. Our new powers, our new ways. Catastrophic risk. But it is managed with the algorithm, every design, every geometry, they always hold. I do remember the old basement. As boys we’d go down there in our grubby shorts and spy on the workers. I remember the day a man in overalls emerged from one of the tunnels, clutching a sack that was writhing with the throws of some living thing. The new drills delving deeper and deeper, unleashing God knew what. One boy had nightmares after that and threw himself from a high window.’
‘A window?’ said C.
‘Fifty years ago they were common. Especially on the upper levels.’
‘I’ve never seen one.’
‘There’s a hatch on the roof too, and ladders descending. There’s been so much expansion of late. Thin wiry extensions to the tower. The old windows were boarded up with the first wild predictions of structural failure. But the algorithm sorted that.’
‘But Gustav, the rats. Tell me more about the rats.’
‘It all changed in ’27 when Chad ordered the basement secured for storage. I suspect a part of him secretly believed in structural failure. He’ll deny it, but the figures in the book can’t be ignored. Couldn’t then, but were, can’t now, but still are. The basement would offer a refuge in the event of failure.
‘But since the drilling the basement became the most complex network of interconnected tunnels and rooms imaginable. Literally thousands of different chambers, dating from different eras. Set up for different power supplies, with different plumbing, faucets, pipes. In starting to explore and clear out the basement on an industrial scale Schwartz-Corp disturbed the rats. Hordes and hordes of rats.’
Gustav had taught C so much about the tower and that day he’d given her the book. She read it twice and it changed everything.
The elevator jolted to a stop.
VI
There was condensation on the glass of Gustav’s door. C wiped her fingers across it and peered inside. The apartment was dark. She opened the door and stepped inside. Dead rats littered the floor and there was stench. But it wasn’t the rats that smelled. Gustav’s large frame lay motionless in the dentist chair he’d taken to napping on. A mug of cold coffee on the spittoon ledge. The surface of the coffee black, reflecting what little light there was. C saw her own reflection, and that of the masked figure behind her. A voice invaded the silence.
‘It’s time. We have come for you.’ The masked figure was now flanked by three rough looking guards.
C knew this moment had been inevitable.
C was blindfolded, carried by strong arms, and taken to a small interrogation room. C’s captors departed. Sitting across a white table from her was Debrovka, Schwartz Corp’s head of legal.
‘Are you here to advise me?’ C asked.
‘No. I am here to prosecute you,’ replied the lawyer. C realized this was the truth.
‘Are you Schwartz Corp’s senior trend analyst?’
‘Deb.’
‘Do you know Mr Gustav Muller?’
‘Come on Deb, you know I do.’
‘He’s dead.’
C felt a strange sense of relief.
‘Nadia Rogers claims that you threatened to kill people this evening.’
‘No. That’s not what I said.’
‘That’s what’s been reported. I am placing you under arrest and charging you with murder. You have the right to say nothing. Under constitutional reform ten zero one one that is your sole right. Do you have anything to say?’
VII
The official record notes that C was silent. In her prison cell, she stood barefoot in a white gown on a cold concrete floor. The ceiling rose high, four triangular panels, sloping and converging in a dome. No doubt the algorithm’s design. She wondered how the walls of the cell would crumble over millennia, where the first cracks might start.
‘What is this?’ the masked figure demanded, a man’s voice. He dropped a stapled sheaf of papers to the floor at her feet. A treatise on the long-term future of Schwartz Corp, with references to dynamics presently in operation. As the document struck the floor the cell shuddered, as if rocked by an earthquake. The pained screech of strained steel pierced the dead air. Then all was still again.
This interrogator saw C’s fear. ‘Don’t worry, the algorithm will intervene. Work crews will be prioritised and redeployed as always.’
‘That’s not what’s worrying me,’ said C.
The masked man snatched with a gloved hand at the collar of her gown, scrunching the stiff starched cloth. He knocked C’s knees from under her with a practised swipe of his boot. Her body folded to the cold stone floor.
‘Why do you persist with this line of thought?’ he asked quietly, kneeling, gesturing to the papers, his lips and hot breath close to her ear. She could smell him and thought, he brushes his teeth, he wears cologne, his uniform is straight, he takes pride in his appearance. He is not like the guards.
C concluded the masked figure is respected, revered as much as feared.
‘Why don’t you forget those calculations?’ A controlled whisper in her ear. ‘It would be easier on all of us. You might even get your job back.’
‘I don’t pick and choose the data,’ she said, ‘What am I supposed to do? Chad set me this task. I…’
‘But you went beyond your remit! A week, a month. Yet here you are writing of decades, millennia.’
‘There is so much to lose,’ she said.
‘Then tell me,’ he said. ‘Hurting you is my role, not my desire.’
C got cautiously to her knees, she opened her mouth but paused.
The interrogator sat on the concrete plinth bed, ‘Go on.’
‘This tower we’re in,’ said C, ‘what does it look like from the outside?’
The masked man considered this strange question. ‘Well it’s… I mean obviously, … it’s…’
‘You see?’
‘See what?’
‘Well is it square or round, or…?’
‘Well…’
‘What does it rest upon? Where does the steel come from?’
These were not questions the interrogator had ever contemplated.
C took a breath and told the interrogator the story of Chad’s rat and the pasta bridge.
When she was done the interrogator nodded and removed the mask. ‘You’re right,’ he said. ‘And it’s obvious really. He can feast, he can walk free, and he can build a bridge. But the sequence matters.’ He paused, thinking, and then added, ‘I need to go, and you should go too.’
The Interrogator closed the door and left.
VIII
The tower shivered. The vibrations and groans of a structure stressed. C stood alone in the cell. She pushed the door. It wasn’t locked.
Forward lagging again, with head down, hungry and cold, she hurried to her office. The book still lay on her desk. C took it under her arm and picked a piece of cake from the drawer.
A crash to one side startled her. She turned to see an iron bar jammed through the wall into her office. Jiggling, it levered an opening, and a long metal strut was pushed through. The algorithm was changing things again, maintaining the fine balance of structural integrity. Endlessly trimming the tower like a wing in flight.
A young girl had poked her head through the door at the sound. She looked at C. C looked back. The child was nine or ten years old. As plaster crashed from the office wall, the girl beckoned C. Book secured under one arm, C followed her into the passageway.
‘Over here, I hide in this cupboard when the builders come,’ said the girl.
With the cupboard door closed it was quiet. The girl turned on a flashlight.
‘Why are you dressed funny?’ she asked looking at the prison gown.
‘It’s a disguise,’ said C, ‘someone dressed me up, so people won’t see who I am.’
‘I see who you are,’ said the girl.
‘Yes, but now you’re in on the secret.’ C smiled, ‘Do you want some cake?’
‘Mummy says I’m not allowed it.’
‘But do you want it?’
The girl nodded several quick nods.
‘What’s your name?’ C asked
‘Abi’
‘Hi Abi, I’m Cassandra. What do you do in here?’
‘I play with my friends.’
‘In the cupboard?’
The girl nodded again, chocolate icing smudged on her nose.
‘Can I give them some cake?’
‘I suppose so, but…’
‘They’re over here.’ The girl had already run deeper in the storage cupboard to a door. She opened the latch and ducked through.
C followed her into the darkness where there was a smell of urine and wet fur.
‘Shh,’ said the girl. ‘Close the door, they’ll come soon. They like it dark.’
‘They?’
‘The rats.’
‘The rats are your friends?’
‘Yes, silly’
‘But wouldn’t you prefer friends you can talk with?’
‘I can talk with the rats’
‘You can talk with the rats?’
‘Of course’
‘What do they say?’
‘Wait and I’ll show you’
‘Look Abi, there’s a big problem. We need to leave this place.’
‘No wait here, the rats have a big problem too. Sometimes I need to call them,’ the girl said and sung a high note. ‘Come on, this way.’
Abi scampered into a shadowy hall accessible through gaps in the structure where a warm draught was blowing. In places the floor was missing too. By some marvel of calculation the algorithm has kept the tower standing for decades as it grew.
The girl was listening now. The hall felt close and hot.
‘Here they come,’ she said, her eyes eager in the faint light.
C heard scuffling and scratching. A chorus of squeaking and peeping followed. A cluster of sleek shadows hustled along a pipe and formed a ring around the girl’s feet. Their chatting high-pitched and constant.
‘Shhh,’ she says to the rats. ‘I’ve brought a friend. Be nice to her.’
There rats sat on their haunches. Their tiny front paws jittered and clawed at the air. Watching with suspicious eyes.
‘He wants to know who you are,’ said Abi pointing to the biggest rat. ‘He wants to know who’s side you’re on.’
The rat squeaked and jittered. Perhaps this girl is lonely thought C. Perhaps she is playing games. Perhaps she is mad.
‘Who is he?’ asked C.
‘He’s their King. He wants to know why you, a big person, will talk to him when the other big people attack and poison his kind?’
‘Tell him I’m sorry for what my people do. Tell him not all of us feel the same way. We don’t all want to kill rats. We’d just rather they didn’t overrun our offices and homes. Those who kill and poison rats do it only to protect their own space.’
The girl whispered to the King. The big grey rat became agitated. He turned around and around on the spot as if chasing his tail. Then he puffed his fur and reared up on his hind paws. He nibbled at the air and hopped up and down.
‘You’ve made him angry,’ said the girl. She watched the rat, listening to his squeaks. ‘Wait, ‘he’s saying more.’
The rat squeaked at length. The girl translating as fast as she could.
‘I am the King of the rats. We lived in those cool quiet tunnels long before your tower arose. At first there was distant rumbling. Our wise elders reflected. They decided that adapting to these vibrations would not do. We were too uncertain of the source, the meaning, what the future held. The elders declared that we must investigate the trembling, and we would have, but the vibrations grew suddenly forceful, and a strange and huge revolving object plundered our great hall. As it withdrew, we saw a tall shaft and light far above us. Investigating this new place, we found the lower chambers of your vast structure. None of us could ever have guessed at the ultimate magnitude of your tower here. For yes, we were beneath the basement of your tower, and we observed your great machines grinding the earth without regard for our tunnels and homes. You drove foundations deep. You set cats and poison upon us. A few of your children heard our pleas, it seemed only they could understand us. But of course, children, though perceptive, lack wisdom and influence. We knew a frontal assault would be futile, so we targeted the weaknesses of your machines. We gnawed cables or wires. For a time, your excavations slowed, but recently you’ve brought more destructive methods. You blast the rock with your fearsome technology and build even greater foundations, in our earth! We have no defence and there was no hope of escape. Until we secured access to the upper floors of your tower.’
IX
C stared at Abi knowing the story could only have come from the rat. She asked, ‘you know how to reach the summit of this tower?’
‘Yes, but we are unable to open the hatch,’ said the Rat King.
In that moment, C foresaw the hatch opening, she had visions of an exodus down endless ladders.
‘Show me the way,’ said C to the rat, ‘I can help you. Abi, find some place safe.’ C handed Abi the book, ‘and take this with you.’
C followed the Rat King. The rats, hordes of them, swarmed from all around and followed the pair. They climbed ladders, walked beams of wood, leaped from girder to girder, swung on dangling cables. Climbing for hours through the maintenance halls of the tower. The horde of rats growing ever larger into a thrashing squealing sea of urgency.
Arriving at the hatch, C was acutely aware that she had never been outside the tower. She wasn’t sure exactly what was outside the tower. She’d heard the stories, read technical reports, and seen drawings. But none of that guaranteed what she might find.
X
C was sweating as she unscrewed the final nut on the hatch and took its weight as it dropped free from the frame. C looked at the ocean of rats below her. Moisture dripped from holes in iron. The rats looked exhausted. C lowered the panel and let it clang to the floor. A blast of heat and wet buffeted her face.
Wiping her face and eyes of hot stinging rain, C hauled herself onto the roof. Around her stood a disparate array of pylons, antennae and an intricate lattice of catwalks. Yet nothing seemed complete. Whole once-towering needles of steel lay strewn, dismantled. They were sparse metallic skeletons. Gaping holes in the roof revealed canyons of woven iron framework plunging dozens of floors into the interior of the tower. Elevator cables hung idle, their carriages removed. Fixtures and struts and even load bearing girders were gone, wrenched from the fabric of the tower and carried off elsewhere.
Soon there were hundreds of rats swarming beside C, then thousands, millions piling across the roof which creaked.
Looking down, C saw that the tower shot magnificently upwards, kilometres from the rocky ground. It was not symmetrical. Huge spindles of parasitic structures clung to each side. Counterweights dangled from crane-like beams, slowly adjusting to maintain balance. Antenna clawed disorganised craving the sky.
Looking to the distance, C could see a vast land stretched to the horizon, resource rich but empty. The tower stood alone. But it stood on an island of rock. The shores of which were bounded all around by a fearsome precipice. The ruins of a half-finished bridge jutted into the abyss, far short of the land around. The frame of the bridge like some decaying edifice, now a dwindling supply of steel to the ever-hungry tower.
Upon the cracked and broken island of rock around the tower, bound by the precipice, lay twisted iron, cracked concrete, burned and blackened piles of rubber. But there was nothing else. No trees, no birds, no water, no space. The precipice lay between the tower and everything else.
Straining under the untold unbalanced weight of the rat hordes, the structure let cry a sudden wrenching wail. The most violent metallic shudder yet. A plea of agony as steel folded upon itself…
XI
‘And this is the truth?’ said Justice Thomas.
‘It is,’ said Everton.
‘Foolish woman. Half our people have perished. Half the tower is lost over the precipice. What did she think she was doing?’
‘I believe she thought she was saving us from an existential threat.’
‘And what do you think?’ said Thomas.
‘I think it was a good plan. But the algorithm didn’t know. It hadn’t predicted the shifting weight of the rats. Nothing like that was in the training data.’
‘You’ve not spoken like this before Everton. What’s changed you?’
‘C’s story in that cell. In a few words she conveyed the essence of our predicament. That one creative act, though imprecise, perhaps because imprecise, did more to change how I think than a hundred dense short-sighted reports.’
The small girl at the back of the courtroom holding her mother’s hand was deep in thought.
She thought, was Cassandra too foolish or just too late?
She thought, I wonder if the chasm is bottomless?
She thought, it is not the tower that needed stability, but the bridge.
She thought, the sequence matters.
She clutched the book in her other hand.
She knew the word now. The Precipice. One day she would read it.
In 1826 Mary Shelly crafted a vision of humanity’s end in ‘The Last Man’. Depicting a world that persists, indifferent to the demise of our species. The end came at the hands a pandemic, spread by the human technologies of trade and news.
Since the construction of nuclear weapons in 1945 humanity has wielded technological power of extreme destruction, and expert consensus is that the greatest threat to humans are humans themselves.
But given that we are the threat, there is also cause for much hope. Humans are self-reflexive and can change behaviour. Technology has raised the standard of living and human wellbeing worldwide, has provided the tools to escape the Covid-19 pandemic, and promises the foundation for a flourishing future.
Provided we govern and wield technology with appropriate wisdom.
The Existential Risk Observatory, founded in 2021 in the Netherlands, is the latest in a series of global institutions concerned for humanity’s future and with a mission to ensure a thriving global society immune from existential threats.
Driven by optimism for our collective future the Observatory convened a conference on existential risks and invited speakers from around the world.
I had the privilege of presenting my take on biological threats, drawing on research I’d undertaken in conjunction with Nick Wilson of the University of Otago, and others, prior to Covid-19, as well as lessons from New Zealand’s experience with Covid-19, and international research on biological threats.
You can watch my presentation by clicking this link (Session two, talk from 25:10, Q&A from 1:08:55).
Below, I’ve provided the full menu of talks at the conference, which includes:
artificial intelligence
climate change
nuclear weapons
biological threats
policy approaches
Existential Risk Observatory (Netherlands) Conference on Existential Risks
25:10 Biological Risks –Matt Boyd (Adapt Research Ltd, New Zealand)
1:26:15 Policy – Rumtin Sepasspour (Cambridge Centre of Study for Existential Risk)
2:52:25 Nuclear Weapons – Susi Snyder (PAX, Nobel Peace Laureate)
3:56:29 Artificial Intelligence Policy – Claire Boine (Harvard & Future of Life Institute)
As Rumtin Sepasspour (Research Affiliate, Cambridge University) noted in his presentation, governments are key stakeholders in the quest for immunity from existential risk, particularly those that arise from accidental or deliberate use of technology. Governments should look at existential risks as a set to be analysed, prioritised and mitigated.
In our quest to understand, prevent, prepare and respond to existential threats every country should hold these meetings of diverse stakeholders to share knowledge and ideas for successfully navigating the period where our technological power outstrips our institutional wisdom.
A new report from the Secretary General of the United Nations ‘Our Common Agenda’, calls on nations to develop foresight and futures capability under an umbrella of coordinated global action.
An very good informed summary and discussion of the UN report can be read here.
Aotearoa/New Zealand needs structured foresight, but a well-resourced foresight and risk ecosystem must be funded to support public sector CEOs in producing newly mandated long-term insights briefings.
Long-term insights briefings
The Public Service Act 2020 requires every departmental chief executive to publish a long-term insights briefing (LTIB) independent of ministers every three years, starting in 2022. These LTIBs should include medium and long-term risks.
The briefings are to be tabled in Parliament so all political parties will have access to their content. Public consultation and extensive feedback is expected. The briefings should be think-pieces that can enhance public debate.
On 1 September 2021, Professor Girol Karacaoglu of Victoria University of Wellington chaired a webinar discussion on these LTIBs. Speaking were:
Wendy McGuinness (founder and CEO of the McGuinness Institute)
Roger Dennis (foresight and innovation consultant)
David Skilling (founding Director of Landfall Strategy Group)
Wendy McGuinness
McGuinness outlined the history of foresight in Aotearoa/New Zealand, noting the previous existence of a Commission for the Future (disestablished in 1982), which she would like to see returned.
She spoke of the purpose of long-term briefings, they should:
Include foresight andlearnings from hindsight
Be filled with curiosity
Question the status quo
But McGuinness also highlighted ways in which the LTIBs could fail to deliver their intended benefits. CEOs can be busy, shy, humble, uncertain, not foresight experts, risk averse, and desire political safety. Such traits could obstruct the process.
The briefings might be delegated downward, thereby failing to tap into CEOs insights. They might be postponed, rushed, lack sufficient consultation and collaboration.
Roger Dennis
Roger Dennis noted the volatile, uncertain, complex and ambiguous (VUCA) nature of the world. This state of affairs generates a lot of noise which we must distil.
Past clear examples of inattention blindness underscore the importance of foresight:
Nokia had one billion customers in 2006, but failed to attend to the threat of the iPhone.
The World Economic Forum’s ‘top 10’ global risks did not include pandemic disease
David Skilling
David Skilling highlighted some small developed countries that have good foresight processes. Aotearoa/New Zealand could perhaps learn from Singapore, Denmark, or Finland.
New Zealand is a unique context, but we don’t have to reinvent the wheel at every step and we should approach LTIBs as an international learning and collaboration exercise.
Skilling distinguished three time horizons, the immediate term, the 5-10 year term and the decades-long term, arguing that the medium horizon is of crucial importance, but the right questions must be posed.
Crucially for LTIBs to succeed, Skilling believes there needs to be Ministerial demand for the insights. Though webinar audience members thought demand could and should come from the public, iwi, DHBs, NGOs and so forth.
In contrast to McGuinness, Skilling thought we should avoid relegating important foresight work to a Commission, and we should build strategic capability across government agencies.
My interpretation
There are many reasons why LTIBs (and similar foresight processes) are essential. Such processes can help identify black elephants (a mix between a black swan and the elephant in the room – think COVID-19), they can help guide big important policy decisions to which they relate.
This is particularly important where there are irreversible decisions, such as decisions pertaining to environmental capital. They can help identify and mitigate large-scale risk (think risks as diverse as climate, biodiversity, biological threats, cyber threats, AI, demographic change, antibiotic resistance, workforce, even volcanism at global choke points), provided they are accompanied by a map of broad strokes solution space to scaffold debate and action.
However, LTIBs will not emerge that are fit for purpose unless there is a sufficient eco-system of foresight resources available to CEOs to aid in their production. Additionally, the LTIBs will not have the desired impact unless they can be digested, aggregated and issues prioritised by a sufficiently competent and apolitical central entity.
Such an entity needs to be deeply involved in the process, guiding CEOs with expertise and providing resources so that LTIBs are aligned with current foresight methods, cover appropriate time horizons, include relevant risks, and are sufficiently creative and curious, or we will merely end up with more of the same. Public, transparent consultation with diverse experts in academia, industry and the NGO sector is of absolute importance.
Part of the aim of such consultation should be to ensure the right questions are indeed being answered. The World Economic Forum’s risk report that omitted pandemics prevented the right questions being asked moving forward.
As Roger Dennis noted, an approximate answer to the right question is better than certainty on the wrong one. People tend to refine what they already know rather than casting the net wider. Swiss emergency management demonstrated this during the cold war with more and more precise models of nuclear fall-out, and an infrastructure programme obsessively focused on underground shelters:
“[W]hen looking back at the broader civil defence programme of the period, it is evident that such calculative fastidiousness did not extend to weighing which threats to its security the Swiss nation should pay attention to in the first place. Absent at this point in time are explicit calculations weighing the risk of nuclear war against a plurality of risks. Where evidence of comparative assessment is to be found, the calculative practices at play appear rather loose, and the object of comparison rather limited” (Deville 2018).
Such myopia is dangerous, as New Zealand’s influenza-only pandemic plan demonstrated through 2020, along with a risk register focussed on short time horizons. What is New Zealand’s plan for volcanism at a global logistics choke point? Logistics are a hot topic in a post-Covid world. Or something much more certain and inevitable like the Superannuation burden of our demographic trajectory?
Such fundamental decisions as what to include and exclude from LTIBs must not prevent appropriate public debate on resourcing and prioritisation. I say include it all, in iterative fashion if the task is too great in a first pass. And then facilitate expert debate and prioritisation of the highlights.
Marketing needed
A programme of marketing is now needed. Stakeholders should be actively primed to give input to the LTIBs, we should expect to be asked. The briefings themselves should be open to wide peer review.
Wendy McGuinness identified five major foresight think pieces that already exist in the public sector, but that these often fly under the radar. Publicization of the LTIBs when they emerge is critical. Ideally, they should be living documents, with a web-portal where stakeholders can leave feedback in ongoing fashion for the next iteration.
It is my view that without critique, peer-review, public input and societal authorization, these reports may simply serve the status quo.
Moral assumptions should be explicit
The reports should explicitly state the values framework within which they are operating. Why were some future possibilities prioritised for elaboration and not others? They should be accompanied by appendices of topics and themes not included, with an explanation of why not. It is one thing to fail to foresee, but to foresee but ignore must be justified to the public. This is a major shortcoming of one of the existing tools for management of future risks, the National Risk Register, which is classified and not open to scrutiny.
An ecosystem is needed with central aggregation
Unlike other countries, New Zealand lacks a surrounding ecosystem of think-tanks, universities, and large companies developing long-term views on a range of subjects.
For the LTIBs to be done well, to overcome siloed orthodoxy and cognitive biases, support for CEOs will be needed. This support needs to be central and apolitical. Commissions are not sufficiently central to the fundamental mechanics of the public sector, can be ignored, poorly funded or disestablished. Central entities such as DPMC, though apolitical in name exhibit features of politicisation, and a lack of transparency.
A Parliamentary Commissioner, with a well-resourced office of talent, answerable to Parliament (with Select Committee oversight), could be tasked with supporting foresight and risk aspects of these processes. Given the major decisions, some irreversible, about the future that could follow the aggregation of LTIBs, there is value in investing in this capability.
The first round of these reports should be written by experienced multidisciplinary teams, include the possible impacts of extreme risks, as well as a search for as yet unidentified problems. High-level mitigation strategies should be proposed for the public to debate.
LTIBs could be a step towards a very positive future for Aotearoa/New Zealand, but only if executed well.
In the wake of the Covid-19 pandemic, everybody now knows that:
Warnings about pandemic disease had been touted for decades
Myriad organisations had called for increased health security funding
The world ignored all these warnings
SARS-CoV-2 emerged in 2019 with dire consequences
The fact that all these warnings were known, yet action was scant, remains difficult to comprehend. Although somewhat perversely, we even knew we would ignore the warnings. Psychological research has shown that these kinds of rare but devastating events are exactly the ones humans tend to overlook. As if to drive this point home, I noted in the news today that a resident of Westport (a New Zealand town flooded by a ‘1 in 100 year event’) even stated that he knew the area had flooded, but thought “the last one was it”.
The ‘unforeseen’ Covid-19 surprise
International organisations such as the UN, WHO, World Bank, and organisations such as the US National Academy of Sciences had made explicit warnings to governments across many years about pandemic and emerging infectious disease risk.
The human and economic impact of pandemic disease had been detailed, and estimated at half a trillion dollarsper year (Fan 2017). The measures the world needed to take to detect, prevent and respond to infectious disease had been widely circulated and all the States Parties to the International Health Regulations had committed to implementing them (few contributed substantial resources and few had succeeded by the time Covid-19 struck).
No country was adequately prepared for Covid-19 (Dalglish 2021). The risk of coronaviruses had not been appropriately understood by governments, and many pandemic action plans (New Zealand’s included) focused solely on influenza.
A coronavirus pandemic simply wasn’t foreseen many would cry. We were struck by a black swan.
Covid-19 was no black swan
Black swans, are outlier events that comes as a surprise, have a major effect, and are inappropriately rationalised after the fact (Taleb, 2007).
However, coronavirus pandemics had been identified as a ‘time bomb’ after SARS 2003, and had been specifically workshopped in 2019 at the ‘Event 201’ pandemic exercise. This exercise involved leaders from a number of public and private global organisations contemplating how to deal with a coronavirus pandemic that kills 65 million people.
This table-top exercise took place in New York on 18 October 2019, when plausibly the first cases of Covid-19 were emerging half a world away. Within six weeks a handful of concerning cases were being discussed with alarm by experts on the ProMED bulletin board.
None of this fits the ‘surprise’ aspect of a black swan.
In the face of Covid-19 New Zealand lacked public health infrastructure (Baker, Wilson, & Woodward, 2017), lacked surge capacity (Skegg, 2021), and decision-makers had not previously contemplated the most effective measures ultimately deployed. These turned out to be border closure and comprehensive managed isolation.
In fact, as far back as 2017 two New Zealand academics (the author included) had started modelling the threshold criteria for when border closure for pandemics might be economically rational (Boyd 2017, 2018, 2019, 2020). We approached individuals at the Ministry of Health with a research proposal only to be told that border closure in a pandemic would never be a policy option and as such no funding could be provided to explore the policy in more detail.
Had these ‘left field’ organisms (coronaviruses!) and mitigation approaches (border closure) been pre-contemplated, then ‘off the shelf’ solutions, or at least solution outlines, might have been available at the time the pandemic struck. Appropriate border policies enacted in time might have prevented the mind-bogglingly expensive lockdowns New Zealand endured, and appropriate MIQ protocols might have prevented the second Auckland lock-down.
Historical myopia slowed New Zealand’s border control action leading to a troubled and porous approach amid inadequate legislation and the deficient public health infrastructure (Skegg, 2021).
Shortcomings were not unique to New Zealand and structural and textual failures in guiding regulations and processes at the international level, namely the International Health Regulations, and the World Health Organization generally, had been criticised, and continue to be criticised (Boyd & Wilson, 2021).
We knew the threat and we knew there would be a striking lack of global coordination. Covid-19, and its global ramifications, was no surprise, and therefore no black swan.
The black elephant
Indeed, the Covid-19 pandemic was a paradigmatic black elephant, a catastrophe that was extremely likely and widely predicted by experts, but ignored or simply unspoken (Asayama 2021).
Gupta describes a black elephant as:
‘an event which is extremely likely and widely predicted by experts, but people attempt to pass it off as a Black Swan when it finally happens. Usually the experts who had predicted the event – from the economic crisis to pandemic flu—go from being marginalized to being lionized when the problem finally rears its head’ (Gupta, 2009).
Knowledge about human cognitive biases explains why we ignore these kinds of risks (Gluckman 2021).
Overall, and painfully, not only was the threat of Covid-19 known, but we also knew that we would ignore it. There existed a myopic focus on day-to-day health needs, health policy that considers only the health sector, a reactive, response-focused approach, and lack of attention to future welfare. In general, a reluctance to address catastrophic risks, yet these kinds of risks harbour almost all the harm.
Escaping black elephants
By definition, information about black elephants is widely understood. To properly prepare for them governments must look both outwardly and inwardly.
Governments must engage experts not just policy wonks
Looking outward, we need to see crowd-sourced solutions, the power of superforecasters must be harnessed, and governments need to enlist assistance engaging in problem-finding, rather than mere problem-solving activities. These tasks will require close engagement with:
experts in academia
industry leaders & technical experts
non-government sectors
creative sectors
Although sensible plans might already be in place, there is always the possibility (or in the case of coronaviruses, probability) that reality will fall beyond the scope of established plans. Red-teaming approaches are needed, experts should be engaged to try to break existing plans. This requires openness and cooperation.
A percentage of preparatory investment should go to diversifying approaches to outlier events, especially when they are inevitable, as is the case with many black elephants. These days a few tens of millions of dollars thrown at understanding these problems, in order to draw the possibility space of mitigation measures, now looks trivial.
Public sector departments must self-critique
Perhaps more important than looking outward is looking inward. Governments must engage in institutional self-reflexivity and this is a process that must be supported from the outside.
Some of the greatest threats are the processes of governance themselves. These processes can become stuck through entrenchment, inertia, historical myopia, status quo, lack of imagination, ignorance, adherence to ‘best-practice’ and corruption by vested interest.
There must be a continual process of self-evaluation and self-critique. In a world of rapidly accelerating technology and human impact, the days of government departments simply justifying post-hoc their pre-formulated plans must end. A radical revision of risk and responsibility is needed, with diverse inputs and ‘crazy ideas’ articulated in detail and held on file for when they are needed.
National and global catastrophic risks must be the purvey of the population not merely the secret notebooks of Cabinet and DPMC spooks.
References
Asayama, S., Emori, S., Sugiyama, M., Kasuga, F., & Watanabe, C. (2021). Are we ignoring a black elephant in the Anthropocene? Climate change and global pandemic as the crisis in health and equality. Sustainability Science, 16(2), 695-701. doi:10.1007/s11625-020-00879-7
Boyd, M., & Wilson, N. (2021). Failures with COVID-19 at the international level must not be repeated in an era facing global catastrophic biological risks. Aust N Z J Public Health, Feb 23. doi:doi: 10.1111/1753-6405.13082
Boyd, M., Baker, M. G., & Wilson, N. (2020). Border closure for island nations? Analysis of pandemic and bioweapon-related threats suggests some scenarios warrant drastic action. Aust N Z J Public Health, 44(2), 89–91. doi:10.1111/1753-6405.12991
Boyd, M., & Wilson, N. (2019). The Prioritization of Island Nations as Refuges from Extreme Pandemics. Risk Analysis, 40(2), 227–239. doi:10.1111/risa.13398
Boyd, M., Mansoor, O., Baker, M., & Wilson, N. (2018). Economic evaluation of border closure for a generic severe pandemic threat using New Zealand Treasury methods. Aust NZ J Public Health, 42(5), 444–446.
Boyd, M., Baker, M., Mansoor, O., Kvizhinadze, G., & Wilson, N. (2017). Protecting an island nation from extreme pandemic threats: Proof-of-concept around border closure as an intervention. PLoS ONE, 12(6), e0178732. doi:10.1371/journal.pone.0178732. eCollection 2017.
Dalglish, S. L. (2020). COVID-19 gives the lie to global health expertise. Lancet. doi:10.1016/s0140-6736(20)30739-x
Fan, V. Y., Jamison, D. T., & Summers, L. H. (2017). The Loss from Pandemic Influenza Risk. In D. T. Jamison, H. Gelband, S. Horton, P. Jha, R. Laxminarayan, C. N. Mock, & R. Nugent (Eds.), Disease Control Priorities: Improving Health and Reducing Poverty. Washington DC: The World Bank.
G20 report shows global pandemic resilience is within reach, but developed countries like New Zealand need to pay our fair share
The G20 Independent Panel’s report ‘A Global Deal for Our Pandemic Age’ finds that US$15 billion per annum could provide some pandemic resilience through interconnected global measures. Our findings suggest another $31 billion is needed annually to support country-specific measures. However, New Zealand’s contribution would be trivial considering it is yet to contribute the expected 0.7% GDP in overseas development assistance.
The world has long known that health security investment is needed
Prior to the Covid-19 pandemic several international organisations provided estimates of how much the world needed to invest in capability and capacity to prevent, detect and respond to biological threats and attain a minimum level of global health security.
These estimates ranged from the very low ($1.9 billion, the World Bank’s lowest estimate) to reasonably substantial ($100 billion for just 67 low- and middle-income countries, by the World Health Organization). Progress had been made through initiatives such as the Global Health Security Agenda (GHSA), via which the USA provided nearly $1 billion in support to 31 low-income countries.
Health security internationally was known to be poor
However, the countries of the world were still nowhere near attaining a minimum level of health security capability or capacity by the time of Covid-19. This was demonstrated by the average global country score of 40.2/100 on the Global Health Security Index (2019), which identified major persisting health security weaknesses, particularly in the domain of ‘health system’ and also with regard to biosecurity and biosafety.
Health security scores did not predict Covid-19 response
Unexpectedly, the distribution of impact of Covid-19 across countries was not explained by GHSI scores. Countries such as the USA and UK suffered greatly yet exhibited the highest health security scores. Other countries, such as Niue, with low scores, remained Covid-free.
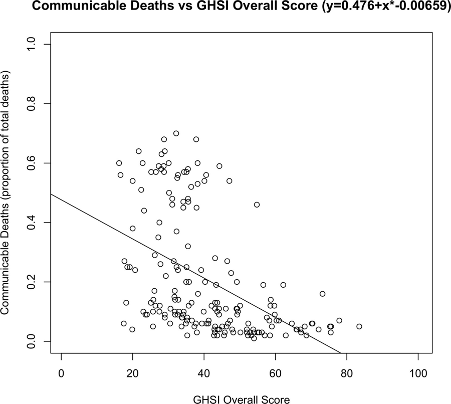
Health security scores are correlated with fewer deaths from communicable disease
That said, our research found a correlation between the proportion of a country’s population dying from communicable diseases, and the GSHI score. This suggests an association with increased health security scores and the ability to deal with internal disease threats.
However, the world as a whole clearly failed to coordinate with respect to Covid-19. There was a lack of integrated disease surveillance, which might have raised the alarm early, there were equipment shortages globally, coordinating global institutions lacked resources to adequately manage a response, and financing to rapidly deploy countermeasures where they were needed was absent.
At least $15 billion per annum is needed for inter-country measures against pandemic disease
In the wake of Covid-19 the G20 commissioned an Independent Panel to report on financing needs that would adequately ensure preparation to meet future emerging disease threats. The Panel identified that the missing pieces of the puzzle are not internal measures by individual countries, but rather coordinating measures and global public goods. Notably, these inter-jurisdiction factors are not assessed by health security metrics such as the GHSI that score individual countries, and it is logically possible (and indeed was the case for many countries) that isolated high scores for GHSI mask a complete lack of international integration across countries’ preparedness measures. It is not surprising, with hindsight, that GHSI failed to track Covid response.
In broad strokes, the G20 Report found that the following measures should be financed:
Global coordination through high-level global governance systems
Global institutions that have adequate and secured funding fit for purpose
Global surveillance systems that are interconnected
Global public goods and financing mechanisms to ensure availability and distribution
The G20 Independent Panel estimates the cost of these measures (and some others) at US$75 billion across five years, or US$15 billion per year. They note that the cost of an event such as Covid-19 is 300-700x this investment. The implication is that the ROI is vast. However, this statistic muddies the picture because the cost of Covid-19 is per event, not per year. If we’re aiming to estimate the cost-effectiveness of an annual investment of $15 billion, we really want to know the annualised cost of (all) biothreats.
Health security investment is associated with increased health security scores and might further reduce death from communicable diseases
In previous research we performed two extrapolations. Firstly, we compared the GHSI scores of countries that had received a share of the United States’ contribution to the GHSA programme. We found that countries receiving this funding scored +6 points higher than matched controls on the 100-point scale. These additional points came at an average cost of US$4.6 million per point. If we aimed to raise all countries to a score of 75/100 this would cost $31 billion and given the relationship between internal communicable disease deaths and GHSI scores (the scatterplot above), this might reduce ordinary communicable disease deaths by 16.7%. Assuming 50% annual ongoing maintenance costs, this programme might cost US$90 billion over five years. We note that this figure is in the same ballpark as the WHO estimates prior to Covid-19.
Global coordination is still needed, and country-specific plus international measures could cost US$33 billion per annum
However, what we’ve learned from Covid-19, and I discussed above, is that the missing piece of the puzzle appears to be global coordinating mechanisms and systems for providing global public goods that can be deployed anywhere and everywhere they are needed, rather than leaving it up to each country to ensure self-contained preparations. This is where the G20’s estimate of a further $75 billion comes in. This requirement must be added to the costs of bringing each country’s internal preparations up to a minimum standard. The total cost might therefore be US$75 billion PLUS US$90 billion, which is US$165 billion over five years, or $33 billion per year.
The return on these investments in health security is likely very good
We can calculate the return on these investments as follows. Our research estimates the annualised cost of all biothreats (including pandemic influenza, SARS, MERS, Zika, Ebola) at US$622 billion. This is excluding Covid-19, which is estimated to cost tens of trillions of dollars, but the inter-covid interval is not clear, so it is hard to annualise the costs across, say a couple of decades. Other estimates have put the costs of biothreats at $1 trillion annually. If we assume even just a 10% reduction in the impact of biothreats due to the measures outlined (eg 1 in 10 pandemics is avoided, or the number of deaths from each is reduced by 10%, thereby saving $62 billion in annual harms) then the ROI is as follows:
The cost of a minimum standard of international health security measures is relatively trivial for developed nations
To put this in perspective, if only the richest billion people on the planet were tasked with paying for this, then New Zealand’s contribution would be $US165 million. Or 0.08% of GDP. Given that the UN recommends that developed nations contribute 0.7% of GDP in development assistance, and given that NZ (in 2019) contributed only 0.28% of GDP, adding this additional contribution is still well within the expectations of New Zealand as a global citizen.
Another way to look at this is at the level of individuals. $33 billion per annum globally is $33 per person for the world’s 1 billion wealthiest people. Health security measures are well within reach for an almost trivial investment.
What New Zealand can do
Advocate for global Heads of States meetings to agree to action on biothreats.
Act to commit the recommended 0.7% of aid internationally by at least doubling present ODA investments and add an additional 0.08% for pandemic preparedness measures, thereby supporting the G20 recommendations.
Enhance our local domestic capabilities and capacities to increase NZ’s and our Pacific neighbours GHSI scores.
Stop the endemic habit of public sector departments justifying status quo preparations, and instead cultivate a norm of engaging in continual problem and risk finding and solutions. Ask (of MIQ, health system, pandemic preparedness, vaccine programmes, public goods, global agreements) how can we make this better? Rather than constantly saying ‘our measures are in line with global best practice’. It should simply be obvious that ‘current best practice’ was inadequate.
Appropriately incorporate biothreat risk into our National Risk Register and publicly communicate the risks and problems to seek additional innovative crowd-sourced solutions.
A minimum level of health security is well within reach globally and developed nations must rapidly finance the measures required. The next pandemic could begin at any time.
Spoiler alert: it has nothing to do with proving the origin of Covid-19, pointing the finger, apportioning blame, reparations, or US-China relations.
The lab leak theory
The lab leak theory, as is now widely understood, is the hypothesis that Covid-19 invaded the human population, not as a result of some ‘natural’ animal-human interaction, but as a result of a coronavirus making its way from laboratory samples directly into the world. The most likely place this might have occurred is at the Wuhan Institute of Virology.
To be clear, the lab-leak theory does not rest on there being malicious intent, or gain-of-function research, or negligence. It is enough that a dangerous pathogen might have accidentally emerged from a high security laboratory to wreak havoc on the world. The lab-leak hypothesis does not depend on human engineering of a virus. A naturally occurring (though no less dangerous) virus could still leak from a lab.
A friend of mine expressed the feeling many people have about Covid-19 origins when she said: “I don’t think it really matters. Pandemics will arise from a variety of sources, what’s more important to focus on if how can we learn (from this experience) how to respond better when they do?”
This is part of the crucial point. But our best response to a pandemic is to prevent them. If we are dismissive of a laboratory origin, then our prevention strategies will overlook prevention at laboratory sites. If the laboratory hypothesis is reasonably plausible, then we ought to invest a reasonable amount in securing laboratories. If we are ever able to elucidate the actual origins of Covid-19 and it was in fact a sequence of events involving a laboratory, then our investment in prevention should specifically target that sequence of hazards.
I personally doubt that we will ever find conclusive evidence of a lab leak. This is partly because the leak may have been a leak of a naturally occurring organism, and partly because any hard evidence in supporting a lab leak has almost certainly been destroyed. We should keep investigating, just in case, but I’m not holding my breath.
The probability of a lab-leak
Without conclusive evidence we must take a probabilistic approach. Authors of one account derived the probability of the Covid-19 pandemic being the result of a lab-leak by imputing known published probabilities across a range of key causative variables. On this principled probabilistic account, the probability of a naturally occurring SARS-like community outbreak originating in Wuhan is 1 in 1000 years, while the probability of a lab-leaked community outbreak occurring in Wuhan is 1 in 833 years. Given that there was in fact a SARS-like community outbreak in Wuhan, one of these must have occurred. This means the probability of a lab-leak origin is 55% and a natural origin is 45%. Even under very conservative assumptions these authors still find 6% probability for the lab leak hypothesis. This is the correct approach to reporting on the origins of Covid-19.
We shouldn’t be pitting one theory against the other to determine certainty, which we may never find, we should be determining probability, which can then guide resource allocation.
Hence the reason why the lab-leak theory is a big deal, and it is a very big deal, is simply because it is plausible, and not only plausible, but perhaps equally likely.
Irresponsible representatives and media
There is almost no greater threat to humanity than a global pandemic. This means that we must avoid them at all costs. Unfortunately, getting to the bottom of the issue has become a partisan football. This is clear when former US President Trump spoke of the ‘China virus’, or through the combative imagery, tone and rhetoric on Sky News Australia when that channel reports on the lab-leak hypothesis.
Much media coverage of the Covid-19 origin story is not helping us prevent future pandemics. In fact, it is probably raising the risk. Too many media outlets are running an attack campaign on China. The effect of this kind of approach is likely to push Chinese officials into defensive mode, counter-offensive mode, and secretive mode. None of this helps us achieve a transparent investigation of the facts. This is a lose-lose strategy, and media outlets running this approach will have the blood of future pandemics on their hands.
Other media outlets are running the opposite campaign. They are minimising the lab-leak theory with faulty logic such as ‘there’s no conclusive evidence for a lab-leak’ (when there’s no conclusive evidence for a natural origin either), or ‘Leading biologist dampens his “smoking gun” Covid lab leak theory.’ Which misses the point that a lab-leak of a naturally occurring organism might not carry a ‘smoking gun’ genetic signature. None of this is helpful.
High-reliability industries and system safety
Many industries depend on ultra high-reliability functioning. These are industries where one failure can have dire consequences. The rate of error needs to be as low as one in a million, or even less. We don’t want any more than one in a million patients to die due to anaesthesia, or one in a million planes to crash, or one in a million nuclear control rods to jam. Ideally the failure rate is even less. In surgery, these are the ‘never events’.
These high-reliability industries, provide a template for the way to investigate causal factors when disaster (or near miss) happens. The process must be a robust, dispassionate, no blame approach. People are error-prone, this is simply a fact of our psychology and biology. Therefore, systems must be engineered to make failure impossible. It is inadequate systems that cause catastrophe because the systems have not adequately protected against error-prone humans.
In laboratory science we never want a dangerous highly communicable organism to infect a human. In fact, the downside is so great (potentially millions if not billions of lives at risk) that we should aim to have complete knowledge of any situations where a laboratory safety failure might possibly have occurred, or is predisposed to occur, or has occurred with 50% probability!
If the lab-leak theory is equally likely to the natural origin theory, then we should assume that there was a lab-leak and spend a decent amount of resource conducting a no-fault investigation into how-possibly it might happen. What causal factors could lead to a lab-leak. This kind of process should draw upon the well-established principles of root cause analysis and failure modes and effects analysis from engineering, as well as human factors principles deployed in high-reliability systems. If any flaw in the laboratory system is identified, then this must be addressed, and the learnings shared with all other labs and also with regulators. All this should occur whether or not we ever find conclusive proof a lab-leak happened.
There should be no witch hunt, there should be no talk of fault and blame and reparations. In fact, there should be a guarantee that no fault will be determined. We want cooperation, transparency and access, but sadly the approach to date has been combative and finger pointing. Representatives’ comments fuel headlines and headlines fuel the agenda of representatives in a vicious cycle. Each actor in this system whether editor or politician has a responsibility for nurturing the conversation in a direction more likely to save future lives than cost them.
Greatest threat to humanity
Covid-19 is, thankfully, a serious but not catastrophic pandemic. Next time we might not be so lucky. An engineered virus, possibly the result of gain-of-function research, could escape a laboratory. It could cause another global pandemic, it could kill a billion people. All this makes the threat from bioengineering a greater, or at least more immediate risk than climate change, a risk equivalent to nuclear war, a risk potentially more imminent than a catastrophic failure of advanced artificial intelligence. Seen in this light the world ought to be far more interested in preventing the next pandemic, far more fastidious about identifying all ways that a virus ‘how-possibly’ might have escaped the Wuhan Institute of virology, and spending far less time and effort waiting for conclusive proof, and seeking to blame, effort that is preventing us preventing the next pandemic.
Even if the probability of a lab-leak at Wuhan is ‘only 6%’, but especially if it is 55%, then decision makers need to pay attention. There is no point waiting for a ‘smoking gun’. Biosafety and biosecurity should be ultra high priority policy domains moving forward.
There is in fact a blueprint for how to begin the process of preventing lab-leaks. The Global Health Security Index (GHSI) prescribes 140 things that countries can do to enhance health security. Many of these items pertain to biosafety and laboratory security, and almost no countries have implemented any of them to date. It is unfortunate that some measures of Covid-19 ‘success’ have not correlated with the GHSI, and hence some researchers have criticised the GHSI’s usefulness. If lab-leak is a live hypothesis, this mindset might mean throwing the baby out with the bathwater.
The Climate Change Commission in New Zealand has recently recommended that changes required to cut emissions to acceptable levels might cost 1.2% of GDP by 2050. At a global level this is US$1 trillion dollars per year. Appropriate investment in biosafety and biosecurity, including contributions to new and needed international organisations probably does not need come anywhere close to this, but such investments are an equal priority given the risks and probabilities involved. It just so happens that US$1 trillion dollars per year is the expected average annual cost of emerging infectious diseases.
Some first steps are obvious, and free. The world banned atmospheric testing of nuclear weapons, and we can ban gain of function research in virology.
Cassandra: True prophecies that were never believed
Despite a WHO-led investigation, compelling evidence on the origin of the SARS-CoV-2 virus remains inconclusive. The WHO investigation concluded in favour of a natural origin, being satisfied that ‘asking whatever questions we wanted’ and obtaining answers to these questions ruled out a laboratory leak. Researchers at the Wuhan Institute of Virology stated that they do not keep similar viruses to SARS-CoV-2, and they have appropriate safety training (while not divulging actual laboratory records).
Skeptics of the natural origin theory, on the other hand, say they wouldn’t trust the outcome of the investigation because it was closely overseen by China’s government. In fact a new report just published in the Bulletin of the Atomic Scientists argues in favour of the lab leak theory citing publicly available records of gain-of-function coronavirus research at the Wuhan Institute of Virology that specifically made use of ‘humanized’ mice, to enhance the ability of the virus to infect human cells. Furthermore, there is some indication that risky work was undertaken not in the strictest ‘BSL 4’ laboratory conditions, but in a more lax BSL 2 environment. The full report in all its forensic detail is available here.
So who is right? Where did SARS-CoV-2 emerge from? When there are competing uncertain hypotheses we might employ a principle of parsimony to infer the correct explanation, or we can use a principle based on prior knowledge of conditions that might be related to the event.
Parsimony: Ockham’s Razor
Ockham’s razor is the principle that when solving a problem (or explaining a pandemic), entities should not be multiplied without necessity. Basically, the explanation that posits the fewest moving parts is likely to be the right one. Did the existence of nature cause a pandemic? Or did the existence of nature AND a virus laboratory in Wuhan cause a pandemic. In this case, parsimony would lead us to conclude that SARS-CoV-2 emerged naturally, the simplest explanation.
Prior probabilities: Bayes’ Theorem
However, there is another approach. Bayes’ Theorem allows for conditioning probabilities on known data points particular to a case of interest, rather than merely on background probabilities. For example, the probability of a coronavirus outbreak across scenarios such as:
in a random city
in Wuhan specifically
in Wuhan given the existence of an Institute of Virology
in Wuhan given the existence of an Institute of Virology that is conducting work on how to modify coronaviruses so that they more easily infect humans
in Wuhan given the existence of an Institute of Virology that is conducting work on how to modify coronaviruses so that they more easily infect humans, and in which it is known that laboratory safety protocols are being violated
We see that scenario (5) posits a lot more entities (an institute, a specific project, particular behaviours, etc) compared to merely ‘nature’ and therefore according to Ockham’s razor such an explanation is manifestly unnecessary to explain the pandemic. However, according to Bayes’ Theorem the base (‘prior’) probability of the pandemic being the result of a lab leak must be massively increased given the additional information contained in (5). Furthermore, if we do not find data points that we would expect to find were the natural outbreak theory true, such as evidence of rapid viral evolution in early cases, or evidence of a natural animal reservoir of SARS-CoV-2, then we must revise downward the probability that natural is the correct explanation (even if it is the most parsimonious).
But have details such as those proposed in the previous paragraph been borne out? The article in the Bulletin of the Atomic Scientists argues ‘Yes’. You can read the full article by clicking the link, but here are two key passages.
“No one has found the bat population that was the source of SARS2, if indeed it ever infected bats. No intermediate host has presented itself, despite an intensive search by Chinese authorities that included the testing of 80,000 animals. There is no evidence of the virus making multiple independent jumps from its intermediate host to people, as both the SARS1 and MERS viruses did. There is no evidence from hospital surveillance records of the epidemic gathering strength in the population as the virus evolved. There is no explanation of why a natural epidemic should break out in Wuhan and nowhere else. There is no good explanation of how the virus acquired its furin cleavage site, which no other SARS-related beta-coronavirus possesses, nor why the site is composed of human-preferred codons. The natural emergence theory battles a bristling array of implausibilities.”
These findings would push a Bayesian to downgrade the likelihood of a natural origin from whatever prior probability was favoured. And then, in research funded by the US National Institute of Health, taking place at the Wuhan Institute of Virology:
“Dr. Shi set out to create novel coronaviruses with the highest possible infectivity for human cells. Her plan was to take genes that coded for spike proteins possessing a variety of measured affinities for human cells, ranging from high to low. She would insert these spike genes one by one into the backbone of a number of viral genomes (“reverse genetics” and “infectious clone technology”), creating a series of chimeric viruses. These chimeric viruses would then be tested for their ability to attack human cell cultures (“in vitro”) and humanized mice (“in vivo”). And this information would help predict the likelihood of “spillover,” the jump of a coronavirus from bats to people… The methodical approach was designed to find the best combination of coronavirus backbone and spike protein for infecting human cells. The approach could have generated SARS2-like viruses, and indeed may have created the SARS2 virus itself with the right combination of virus backbone and spike protein… It cannot yet be stated that Dr. Shi did or did not generate SARS2 in her lab because her records have been sealed, but it seems she was certainly on the right track to have done so.”
These facts, along with evidence pointing to unsafe laboratory practices detailed in the Bulletin of the Atomic Scientists article raise the probability of the less than parsimonious explanation.
US Intelligence and Donald Trump
Furthermore, the laboratory project of concern was being undertaken in Wuhan, but was funded by the US NIH. This new knowledge explains some previously puzzling facts. The lab-origin theory (and possible early illnesses affecting lab staff in November 2019 as detailed in the Bulletin) is consistent with the US intelligence services claim that there were cases of SARS-CoV-2 prior to December 2019, as detailed here. President Trump then cited the lab theory as his favoured theory based on the intelligence he had received (see here), and he used a PR tactic of referring to SARS-CoV-2 as ‘the China virus’ repeatedly. This could all have been dismissed as it was at the time as Republican posturing. It seemed unusual at the time that if US intelligence or Trump had a smoking gun implicating the Wuhan Institute of Virology, then given their rivalry with China they would have revealed this to the world. As it transpires, the coronavirus project at the Wuhan Institute of Virology was funded by the US NIH. Had intelligence officials, or Trump himself in the interests of political point scoring made their information public, then the US would have immediately been implicated. The lab-leak theory now explains something that was previously unexplained. Explainability is another marker of a correct hypothesis.
Mitigation Matters
Why does it matter where SARS-CoV-2 originated from, given that it is now here, and everywhere on Earth? The list of plausible origin stories for a situation like COVID-19 has immense practical importance. Because to mitigate such events in the future, we must ensure that at least some of the measures we deploy target the actual sequence of events. If the ‘most likely’ explanation is a natural origin, and we target all future measures at reducing the probability of natural origin, and yet in fact, the origin was anthropogenic, then we may miss the opportunity to lower the risk of anthropogenic catastrophe in the future. Certainty and zealous defence of parsimonious explanation is an extremely risky policy strategy.
Prevention policy and the lose-lose square
In global risk reduction there are often difficulties getting buy-in for prevention, safety and preparedness measures because vested interests obstruct the process (think fossil fuels and carbon emissions). Some policies aimed at mitigation result in someone or some state winning and someone else losing. There may be fear of economic contraction or first mover disadvantage in some domain. Yet in the complex game-theoretic melee of international relations there are lose-lose positions, where no one wins from the status quo. This is where leverage might be gained to help reduce global catastrophic risk. There is a prima facie case, enhanced by the discussion above, that gain-of-function research on viruses capable of infecting humans sits entirely in the lose-lose square. By banning such research we can reduce the risk of technological catastrophe.
Science advances ‘Funeral by funeral’
The article in the Bulletin of the Atomic Scientists made me think of a quote by Max Planck. To paraphrase, ‘science progresses one funeral at a time’. Planck’s idea was that scientists are a dogmatic breed and the only way falsehoods vanish is through the death of their proponents. However, given today’s scenario, this maxim can be interpreted a different way. The ongoing litany of technological catastrophes (think the Bhopal disaster, Banqiao dam failure, Chernobyl disaster, recent ‘Irresponsible’ rocket debris) seem to indicate that death must occur for safety and wisdom to truly advance. It is the funerals of ordinary citizens, victims of hubris (or gain-of-function research), whose deaths may (or may not) lead to safer systems and more precaution. Science may well advance ‘funeral by funeral’.
Greek Tragedy
As one public health physician has recently put it: “The irony is that it was US-funded research, and like a Greek tragedy may have created the end it was seeking to avoid: a pandemic.” Whether SARS-CoV-2 emerged from a laboratory or not, we must be sure that we do not move forward creating the very ends that we seek to avoid.
Biological threats far worse than Covid-19 are possible, even likely.
Governments should consider worst case scenarios and contingencies.
Risks should be catalogued and published in a form that expresses expected utility loss (probability x impact).
In an existence threatening scenario, Australia and New Zealand are the island refuges most suited to seal borders to safeguard humanity.
Many practical steps can be taken to ensure that island refuges are a viable option of last resort if a catastrophic biothreat arises.
Island refuges in some geographic locations might offer additional resilience against nuclear winter.
It’s no longer surprising news that COVID-19 may be a warning shot that provides humanity the chance and the motivation to address some of the many catastrophic global risks. Our latest research paper explains the rationale and practicalities of island refuges as mitigation.
Biological Threats
Pandemic viruses with high case fatality could potentially infect a majority of the population. Deliberate biological events (DBEs) have occurred before (Millet & Snyder-Beattie, 2017a), will likely occur again, and could pose catastrophic or existential threat to humans. With rapidly advancing biotechnology it is conceivable that an engineered virus might combine features of very high transmissibility and very high case fatality. Multiple engineered viruses could conceivably be deployed simulataneously to achieve close to 100% fatality risk in human populations (Turchin & Denkenberger, 2018). Finally, new technologies such as artificial intelligence could amplify biothreats in many ways (O’Brien & Nelson, 2020).
The threat of a DBE could be partly driven by a search for ‘winter safe’ deterrence (Baum, 2015), or for cheaper alternatives (relative to nuclear weapon arsenals) to nuclear mutually assured destruction. These risks are amplified because the Biological Weapons Convention (BWC) has no verification system (Dando, 2016), and has been violated in the past (Gronvall, 2018). It would only take one unanticipated or accidental event for a bioweapon (or laboratory accident) to become a catastrophic threat.
These risks should ideally be expressed by governments in terms of expected utility loss (ie probability x impact). For example, hypothetically:
A 20% probability per annum of an Ebola outbreak that kills 10,000 people, for which the expected utility loss is 2,000 deaths per annum.
A 1% probability per annum of a catastrophic biological attack that kills 20,000,000 people, for which the expected utility loss is 200,000 deaths per annum.
Clearly the second threat would be the larger risk and at least some analysis and policy resources should be tasked with better understanding risks like it and how to mitigate them.
Resources could be allocated to risk mitigation in proportion to the expected utility loss, keeping in mind that some mitigation measures will address multiple risks.
We need options of last resort
No preventive or resilience strategy is foolproof. An anthropogenic pandemic of existential magnitude is probably more likely than a naturally occurring one, and the world ought to pursue technologies that ensure safety.
However, last lines of defense may be required, such as refuges. If an island nation closed its borders quickly enough, allowing no one at all in, it could keep the threat at bay, thereby protectively sequestering its population and preserving technological know-how.
Island Refuges
Image source: iStock
Many islands might unintentionally act as refuges where humanity survives, such as North Sentinel Island which harbours a population that vigorously rejects outsiders. However, many such islands do not harbour the materials and know-how to preserve a technologically flourishing civilisation.
Our new research paper poses the question, ‘which islands are most suited to safeguard a population of humans in order that a technologically flourishing global civilisation might be restored after a catastrophic pandemic?’
We explore this question in depth and determine it is Australia, New Zealand and Iceland, but that none of these three islands is yet fully prepared to play such a role in protecting human existence as we know it. Given Australia and New Zealand’s proximity and close relationship there is potential to cooperate on such a project, especially given there is redundancy with four potential island refuges (Australian mainland, Tasmania, North Island and South Island of New Zealand).
COVID-19 taught us that pandemics may reach many remote islands only after some delay, giving such islands a chance to successfully close their borders and keep the disease out. We also know that there were many disruptions to trade and that such disruptions would only be worse in a more severe pandemic. Disruption could be total in a catastrophic situation.
Preparations should be a mixture of specific anticipatory actions, and more generalist responses for all kinds of scenarios.
Refuge preparations
In order to ensure that an island can survive intact through the catastrophe a number of aspects of self-sufficiency and security need to be developed ahead of time. For example:
Governments should articulate these risks, and possible mitigation measures, crowdsource additional strategies, and begin to evaluate the rationale and priority of various preparations.
Effective military and/or police capability may be needed to repel those determined to try to reach the refuge (who might bring disease with them). This is a weakness many small islands face, however military technology is rapidly becoming cheaper, smaller, more versatile, and autonomous. Still, it would be more ideal for the global community to discuss and recognise refuges ahead of time, and coordinate, perhaps via a treaty or UN resolution, to leave the refuge island(s) alone should a catastrophic pandemic arise. The future of humanity could depend on it.
Nuclear winter
Robbie Norman: Getty Images
Finally, some refuges might help mitigate nuclear winter. The threat of nuclear war persists. A small-scale war between India and Pakistan could have dramatic implications for global agricultural productivity threatening mass starvation (Toon et al., 2019). A limited nuclear war (<1% of the world’s arsenal) could disrupt the climate for 5-10 years, especially above latitude 30 degrees north (Jagermeyr et al., 2020). A larger nuclear war between the US and Russia could lead to below freezing summer temperatures over much of the northern hemisphere (Coupe, Bardeen, Robock, & Toon, 2020). Large scale nuclear war could be catastrophic with the possibility of human extinction, although there would likely be some survivors notably ‘in Australia and New Zealand’ (Robock, 2010). Supervolcanic or asteroid/comet impact winter may have similar effects (Rampino, 2011; Vellekoop et al., 2014), perhaps, too, a geoengineering catastrophe (Dykema, Keith, Anderson, & Weisenstein, 2014).
This means that it might be sensible for Australia and New Zealand to also consider what might mitigate nuclear winter situations as well. There may be some substantive overlap in resilience preparations for nuclear war and for catastrophic biological risks. This is because we can confront nuclear winter by increasing humanity’s resilience to it (Baum, 2016). In the context of a global nuclear war, island refuge status might be imposed involuntarily.
Island nations such as New Zealand could: stockpile food (including alternative sources) (Martinez et al., 2020), water, sunscreen, fuel, and medical supplies; shielding against UV radiation; and secure telecommunications against electromagnetic pulses or loss of cloud connectivity (Baum, 2016).
The reverse of winter scenarios, extreme global warming, is another catastrophic scenario (albeit probably over a longer timeframe), and if the process is reversible then Iceland could potentially harbour a population safely until the threat has passed.
Amplifying risk factors
There are many other considerations that might help or hinder the functioning of a refuge. The 2021 US Intelligence Global Trends Report, warns of the potential fragmentation of societies and the global order, with the possibility of international trade disruption, groups of countries creating online enclaves, and eroded civic cohesion. This is important because social factors such as the degree of societal ‘tightness’ or ‘looseness’ have been correlated with better and worse Covid-19 outcomes. Mechanistic modelling shows how tightness arises in high threat environments because it’s an advantage. Tight countries do better in threat situations and this only enhances the concerns raised in the US intelligence report. It seems some kinds of social structures and interactions are worth nurturing and other trends must be overcome.
Government action is needed
Governments should invest in teams analysing these very large scale threats and trying to determine with more certainty the expected utility loss. This would allow them to publish risk registers, invite crowd-sourced (public sector, business, civil society) input about mitigation strategies, and to rationally prioritise investment in the context of competing demands. Some necessary preparations might be intergenerational human resilience projects.
New Zealand should up its game in risk identification, analysis, and prevention. This is the key message from former GNS principal scientist Kelvin Berryman when discussing a new risks report. He told the Listener, ‘New Zealand is still creating its own disasters waiting to happen.’
The risks report in question was published in April 2021 by former Chief Science Advisor Peter Gluckman and co-author Anne Bardsley. It details New Zealand’s need to address ‘uncertain but inevitable’ risks. The report has garnered media attention such as RadioNZ’s coverage here, and the feature in the Listener available here (paywalled).
The general thrust of ‘Uncertain but Inevitable’ is that governments are responsible for keeping people safe, the New Zealand government has developed a National Risk Register, which allegedly includes maximum credible threats, however this is kept secret when it ought to be public, and that much more institutional transparency and accountability of risk assessment are needed. There should be an apolitical focus on high-impact risks that overcomes three particular failures: (1) risk identification, assessment and communication, (2) human factors (especially issues of cognitive biases), and (3) policy/political dimensions.
I certainly applaud the efforts to improve the scale, scope and transparency of risk analysis in New Zealand. A few additional points warrant mention:
Firstly, it is very notable that the former Chief Science Advisor is critiquing the National Risk Register, one supposes that he was privy to at least some of its contents in his former official capacity, and if he feels the register and/or risk processes surrounding it in Aotearoa/New Zealand are inadequate then we should certainly take note.
Second, the focus on ‘uncertain but inevitable’ risks is surely too narrow. The Listener piece states that a spokesperson for the Prime Minister said, ‘New Zealand had a good track record of identifying and managing risks and was committed to ensuring public discussion about nationally significant risks.’ However, New Zealand’s approach to risks has traditionally been a reactive one. Even forward-looking endeavours like EQC are designed for the aftermath. A track record, even a good one, is not necessarily good for unprecedented and unexpected risks. Notably, our ‘successes’ with Covid-19, the Christchurch earthquake and so on, were with regard to risks that were neither unprecedented, nor unexpected. What about emerging risks such as biological engineering, misaligned artificial intelligence, solar geoengineering, rising digital totalitarianism, newly discovered risks from space, and the established but unaddressed risks of nuclear, volcanic and asteroid/comet induced winters, let alone technological risks yet to be identified.
Thirdly, the Listener reported that the authors of ‘Uncertain but Inevitable’ believe it would be theoretically possible to have an all-encompassing risk register, however, they felt that such a register could overwhelm its audience, or result in generic or vague risks. I would counter this point by saying that the point of a risk register is to formalise analysis, to be sure the assessment is systematic and comprehensive. But the register needs to record dimensions beyond the traditional coarse ‘likelihood’ and ‘magnitude’ categories. By adding best probability estimates, best impact on life-years and the economy estimates, considerations of tractability, lists of possible interventions and best estimates of cost-effectiveness (all constantly updated as new information comes to hand), then risks can be ranked by expected annual utility loss. A risk budget can be determined, and this budget allocated to the highest priority risks. It may be that the most important risks are not those that we traditionally pour investment into, such as road safety or flood banks, but rather risks such as the next Covid-19 or a nuclear winter. That remains to be determined by the process just outlined. The register would not be overwhelming if we start by addressing the Top 10 risks.
Fourthly, Berryman is cited in the Listener article as saying that we need more and better science communication. There is plenty of knowledge and research about risks, but this doesn’t always find its way into public policy. This is something I completely agree with and at Adapt Research we hope to initiate a New Zealand Human Futures Forum (currently a funding application is under consideration), which would focus on nurturing discussion and information sharing about global catastrophic and existential threats in a way that is relevant to Aotearoa/New Zealand. This risk category is notably absent from almost all risk policy work. We have previously noted this omission at the level of the UN, and locally in the domains of artificial intelligence and catastrophic biological threats. And yet, when the approach taken in point three above is deployed, such risks may be the most rational ones to address.