

G20 report shows global pandemic resilience is within reach, but developed countries like New Zealand need to pay our fair share
The G20 Independent Panel’s report ‘A Global Deal for Our Pandemic Age’ finds that US$15 billion per annum could provide some pandemic resilience through interconnected global measures. Our findings suggest another $31 billion is needed annually to support country-specific measures. However, New Zealand’s contribution would be trivial considering it is yet to contribute the expected 0.7% GDP in overseas development assistance.
The world has long known that health security investment is needed
Prior to the Covid-19 pandemic several international organisations provided estimates of how much the world needed to invest in capability and capacity to prevent, detect and respond to biological threats and attain a minimum level of global health security.
These estimates ranged from the very low ($1.9 billion, the World Bank’s lowest estimate) to reasonably substantial ($100 billion for just 67 low- and middle-income countries, by the World Health Organization). Progress had been made through initiatives such as the Global Health Security Agenda (GHSA), via which the USA provided nearly $1 billion in support to 31 low-income countries.
Health security internationally was known to be poor
However, the countries of the world were still nowhere near attaining a minimum level of health security capability or capacity by the time of Covid-19. This was demonstrated by the average global country score of 40.2/100 on the Global Health Security Index (2019), which identified major persisting health security weaknesses, particularly in the domain of ‘health system’ and also with regard to biosecurity and biosafety.
Health security scores did not predict Covid-19 response
Unexpectedly, the distribution of impact of Covid-19 across countries was not explained by GHSI scores. Countries such as the USA and UK suffered greatly yet exhibited the highest health security scores. Other countries, such as Niue, with low scores, remained Covid-free.

Figure source: Baum et al 2021 (BMJ, 29 Jan)
Health security scores are correlated with fewer deaths from communicable disease
That said, our research found a correlation between the proportion of a country’s population dying from communicable diseases, and the GSHI score. This suggests an association with increased health security scores and the ability to deal with internal disease threats.
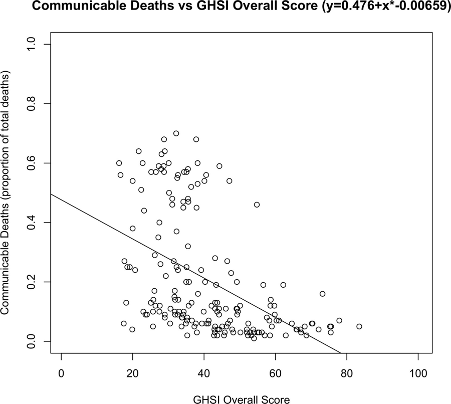
Figure source: Boyd et al. 2020 (BMJ Global Health).
Global coordination was lacking prior to Covid-19
However, the world as a whole clearly failed to coordinate with respect to Covid-19. There was a lack of integrated disease surveillance, which might have raised the alarm early, there were equipment shortages globally, coordinating global institutions lacked resources to adequately manage a response, and financing to rapidly deploy countermeasures where they were needed was absent.
At least $15 billion per annum is needed for inter-country measures against pandemic disease
In the wake of Covid-19 the G20 commissioned an Independent Panel to report on financing needs that would adequately ensure preparation to meet future emerging disease threats. The Panel identified that the missing pieces of the puzzle are not internal measures by individual countries, but rather coordinating measures and global public goods. Notably, these inter-jurisdiction factors are not assessed by health security metrics such as the GHSI that score individual countries, and it is logically possible (and indeed was the case for many countries) that isolated high scores for GHSI mask a complete lack of international integration across countries’ preparedness measures. It is not surprising, with hindsight, that GHSI failed to track Covid response.
In broad strokes, the G20 Report found that the following measures should be financed:
- Global coordination through high-level global governance systems
- Global institutions that have adequate and secured funding fit for purpose
- Global surveillance systems that are interconnected
- Global public goods and financing mechanisms to ensure availability and distribution
The G20 Independent Panel estimates the cost of these measures (and some others) at US$75 billion across five years, or US$15 billion per year. They note that the cost of an event such as Covid-19 is 300-700x this investment. The implication is that the ROI is vast. However, this statistic muddies the picture because the cost of Covid-19 is per event, not per year. If we’re aiming to estimate the cost-effectiveness of an annual investment of $15 billion, we really want to know the annualised cost of (all) biothreats.
Health security investment is associated with increased health security scores and might further reduce death from communicable diseases
In previous research we performed two extrapolations. Firstly, we compared the GHSI scores of countries that had received a share of the United States’ contribution to the GHSA programme. We found that countries receiving this funding scored +6 points higher than matched controls on the 100-point scale. These additional points came at an average cost of US$4.6 million per point. If we aimed to raise all countries to a score of 75/100 this would cost $31 billion and given the relationship between internal communicable disease deaths and GHSI scores (the scatterplot above), this might reduce ordinary communicable disease deaths by 16.7%. Assuming 50% annual ongoing maintenance costs, this programme might cost US$90 billion over five years. We note that this figure is in the same ballpark as the WHO estimates prior to Covid-19.
Global coordination is still needed, and country-specific plus international measures could cost US$33 billion per annum
However, what we’ve learned from Covid-19, and I discussed above, is that the missing piece of the puzzle appears to be global coordinating mechanisms and systems for providing global public goods that can be deployed anywhere and everywhere they are needed, rather than leaving it up to each country to ensure self-contained preparations. This is where the G20’s estimate of a further $75 billion comes in. This requirement must be added to the costs of bringing each country’s internal preparations up to a minimum standard. The total cost might therefore be US$75 billion PLUS US$90 billion, which is US$165 billion over five years, or $33 billion per year.
The return on these investments in health security is likely very good
We can calculate the return on these investments as follows. Our research estimates the annualised cost of all biothreats (including pandemic influenza, SARS, MERS, Zika, Ebola) at US$622 billion. This is excluding Covid-19, which is estimated to cost tens of trillions of dollars, but the inter-covid interval is not clear, so it is hard to annualise the costs across, say a couple of decades. Other estimates have put the costs of biothreats at $1 trillion annually. If we assume even just a 10% reduction in the impact of biothreats due to the measures outlined (eg 1 in 10 pandemics is avoided, or the number of deaths from each is reduced by 10%, thereby saving $62 billion in annual harms) then the ROI is as follows:
(US$62 billion – US$33 billion) / US$33 billion = 88% ROI
If we reduce harms from biothreats by 50% then the ROI is:
(US$311 billion – US$33 billion) / US$33 billion = 842% ROI
The cost of a minimum standard of international health security measures is relatively trivial for developed nations
To put this in perspective, if only the richest billion people on the planet were tasked with paying for this, then New Zealand’s contribution would be $US165 million. Or 0.08% of GDP. Given that the UN recommends that developed nations contribute 0.7% of GDP in development assistance, and given that NZ (in 2019) contributed only 0.28% of GDP, adding this additional contribution is still well within the expectations of New Zealand as a global citizen.
Another way to look at this is at the level of individuals. $33 billion per annum globally is $33 per person for the world’s 1 billion wealthiest people. Health security measures are well within reach for an almost trivial investment.
What New Zealand can do
- Advocate for global Heads of States meetings to agree to action on biothreats.
- Act to commit the recommended 0.7% of aid internationally by at least doubling present ODA investments and add an additional 0.08% for pandemic preparedness measures, thereby supporting the G20 recommendations.
- Enhance our local domestic capabilities and capacities to increase NZ’s and our Pacific neighbours GHSI scores.
- Stop the endemic habit of public sector departments justifying status quo preparations, and instead cultivate a norm of engaging in continual problem and risk finding and solutions. Ask (of MIQ, health system, pandemic preparedness, vaccine programmes, public goods, global agreements) how can we make this better? Rather than constantly saying ‘our measures are in line with global best practice’. It should simply be obvious that ‘current best practice’ was inadequate.
- Appropriately incorporate biothreat risk into our National Risk Register and publicly communicate the risks and problems to seek additional innovative crowd-sourced solutions.
A minimum level of health security is well within reach globally and developed nations must rapidly finance the measures required. The next pandemic could begin at any time.
